Castagna Giona, Ippolito Silvia, Cassibba Sara, Cortesi Liana, Costi Emanuele, Harb Ahmad, Lanterna Luigi Alberto, Sicignano Angelo Mirco, Trevisan Roberto, Rossini Alessandro
Endocrinology and Diabetes Unit, ASST Papa Giovanni XXIII, Bergamo, Italy.
Department of Medicine and Surgery, University of Milano Bicocca, Milan, Italy.
Pituitary. 2025 May 6;28(3):56. doi: 10.1007/s11102-025-01520-5.
Growth hormone (GH) and insulin-like growth factor 1 (IGF-1) are critical regulators of renal development and function. Acromegaly, characterized by chronic GH hypersecretion, leads to renal hypertrophy and glomerular hyperfiltration. While immediate treatment of acromegaly mitigates hyperfiltration, the long-term risk of renal damage in treated patients remains unclear. Our study aimed to assess renal function over time in patients with acromegaly who were followed long-term at our institution.
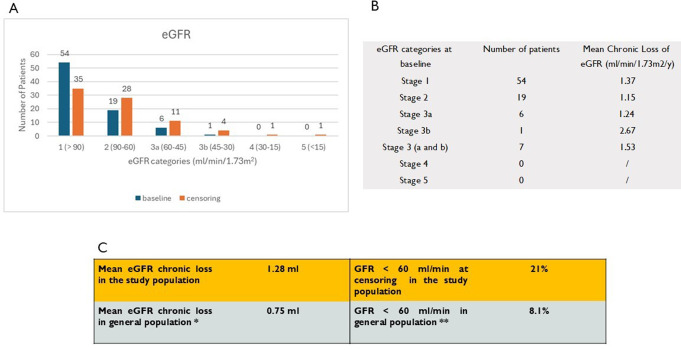
This study analyzed 80 patients with acromegaly from a single center. Creatinine values were recorded to assess kidney function before and after treatment. The estimated glomerular filtration rate (eGFR) was calculated using the CKD-EPI 2021 formula. eGFR variations were evaluated over the first 12 months after treatment (acute slope) and during long-term follow-up with a mean duration of 11.28 years (chronic slope). Descriptive statistics and multivariable regression analyses were performed.
Among the 80 patients (43.7 years, 46 male), 51 underwent surgery (11 of whom also received subsequent radiotherapy), while 29 received exclusively medical therapy. Comorbidities included diabetes (31.25%) and hypertension (65%). eGFR decreased acutely after treatment in all groups, with a more pronounced decline in surgically treated patients (mean - 15.15 mL/min/1.73 m²; p = 0.042). The mean chronic eGFR loss was - 1.28 mL/year, with age (OR 1.09 per year) and diabetes (OR 5.66) significantly associated with a greater decline in eGFR (p < 0.01).
Renal hyperfiltration in acromegaly tends to normalize following treatment, with a more rapid response observed in patients who undergo surgery. Chronic kidney disease is highly prevalent in acromegaly and is closely linked to diabetes, which further contributes to the increased cardiovascular risk seen in these individuals.
生长激素(GH)和胰岛素样生长因子1(IGF-1)是肾脏发育和功能的关键调节因子。肢端肥大症以慢性GH分泌过多为特征,可导致肾脏肥大和肾小球高滤过。虽然肢端肥大症的即时治疗可减轻高滤过,但治疗患者肾脏损害的长期风险仍不明确。我们的研究旨在评估在我们机构长期随访的肢端肥大症患者的肾功能随时间的变化情况。
本研究分析了来自单一中心的80例肢端肥大症患者。记录治疗前后的肌酐值以评估肾功能。使用CKD-EPI 2021公式计算估计肾小球滤过率(eGFR)。在治疗后的前12个月(急性斜率)和平均持续时间为11.28年的长期随访期间(慢性斜率)评估eGFR变化。进行了描述性统计和多变量回归分析。
在80例患者(43.7岁,46例男性)中,51例接受了手术(其中11例还接受了后续放疗),而29例仅接受药物治疗。合并症包括糖尿病(31.25%)和高血压(65%)。所有组在治疗后eGFR均急性下降,手术治疗患者下降更为明显(平均-15.15 mL/min/1.73 m²;p = 0.042)。慢性eGFR平均每年下降-1.28 mL,年龄(每年OR 1.09)和糖尿病(OR 5.66)与eGFR下降幅度更大显著相关(p < 0.01)。
肢端肥大症中的肾脏高滤过在治疗后趋于正常化,手术患者的反应更快。慢性肾脏病在肢端肥大症中非常普遍,并且与糖尿病密切相关,这进一步导致了这些个体心血管风险的增加。