Gunzinger Jeanne Martine, Palmer Sarott Seraina, Meier Fabio, Böni Christian, Kitay Alice, Simonsz-Tóth Brigitte, Gerth-Kahlert Christina
Department of Ophthalmology, University Hospital Zurich, University of Zurich, Frauenklinikstrasse 24, Zurich, 8091, Switzerland.
Department of Paediatric Rheumatology, University Children's Hospital Zurich, Zurich, Switzerland.
J Ophthalmic Inflamm Infect. 2025 May 8;15(1):43. doi: 10.1186/s12348-025-00458-w.
Paediatric uveitis treatment recommendations suggest a step-up treatment approach starting with topical treatment, followed by antimetabolites and thereafter biologics. With this study, we are investigating the safety and efficacy of the current treatment approach in a large cohort.
Single center retrospective study. Patients with non-infectious uveitis under the age of 18 years at first presentation, between January 2012 and June 2022, were eligible for inclusion. Data extracted from the electronic health records included age at first presentation, sex, involved eye segment, visual acuity (VA), complications, associated systemic disease, treatments, and number of consultations. Cases were grouped according to their final treatment regime (topical only, methotrexate, TNF alpha inhibitor, other). VA outcome, treatment response, adverse events, and frequency of consultations were evaluated. The study was approved by the local ethics committee.
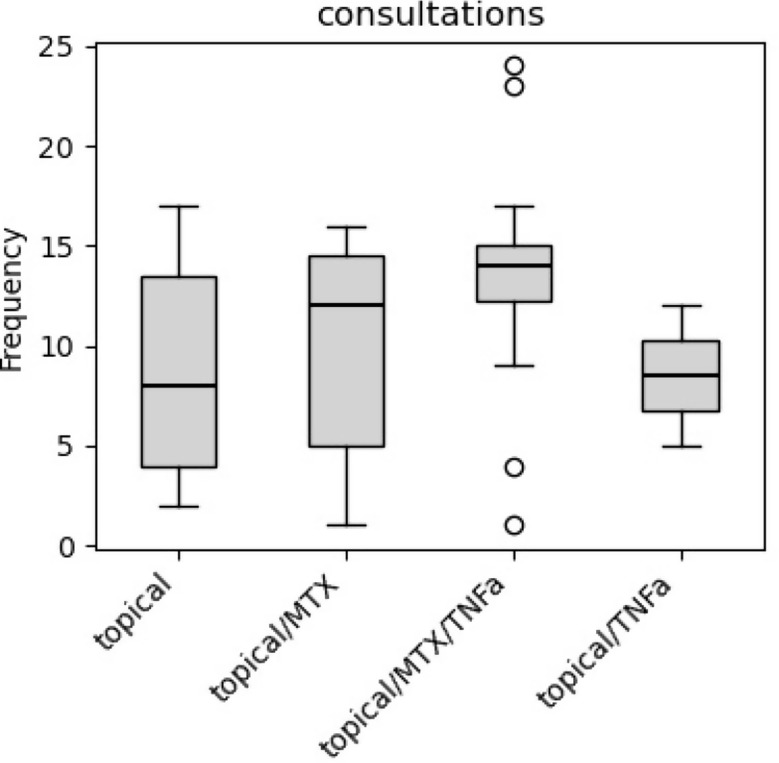
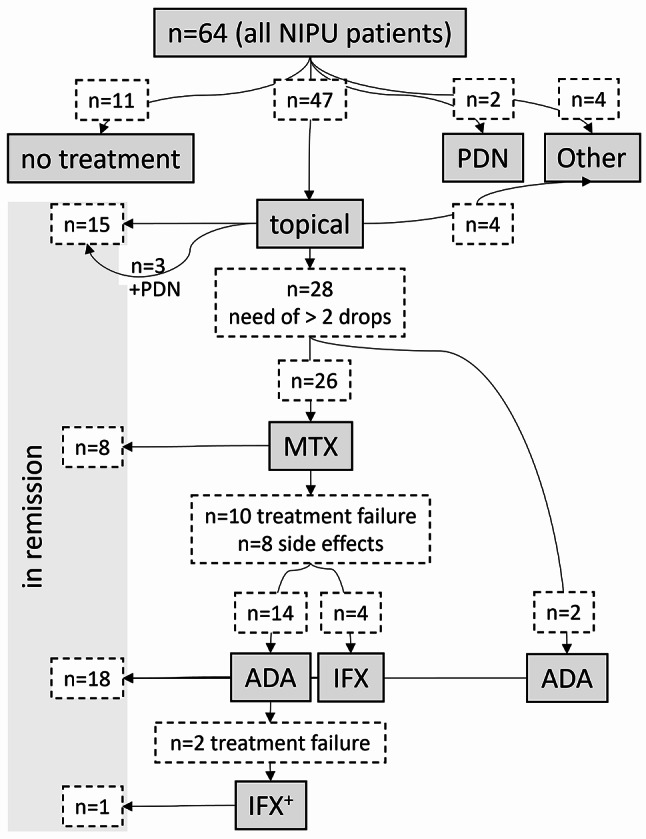
64 non-infectious paediatric uveitis cases were included. Age at first diagnosis ranged from 2 to 17 years, with a two-peak distribution, 52% were male. Anterior uveitis was the most common presentation, followed by intermediate uveitis, posterior uveitis, and panuveitis. Topical treatment achieved remission in 23%, anti-metabolites in 12%, and escalation to TNF alpha inhibitors in 30%. Alternative treatments or observation only were documented in 16% and 17%, respectively. Median duration from first presentation to the start of anti-metabolite or TNF alpha inhibitor were 115 days and 269 days, respectively. There was a median of eight consultations during the first year of follow up. Frequency of consultations during the first year increased with every treatment escalation. VA outcome did not differ between the different treatment groups.
The step-up treatment approach shows a safe profile in regards to VA outcome. Methotrexate presents a high rate of treatment failure and adverse effects. Adalimumab and infliximab are effective and safe. Timely treatment escalation might lower treatment burden for affected children, their families, and health care providers.
儿童葡萄膜炎治疗建议提出一种逐步升级的治疗方法,从局部治疗开始,接着使用抗代谢药物,然后是生物制剂。通过本研究,我们正在调查当前治疗方法在一大群患者中的安全性和有效性。
单中心回顾性研究。2012年1月至2022年6月首次就诊时年龄在18岁以下的非感染性葡萄膜炎患者符合纳入标准。从电子健康记录中提取的数据包括首次就诊年龄、性别、受累眼段、视力(VA)、并发症、相关全身性疾病、治疗方法以及会诊次数。病例根据其最终治疗方案(仅局部治疗、甲氨蝶呤、肿瘤坏死因子α抑制剂、其他)进行分组。评估视力结果、治疗反应、不良事件以及会诊频率。该研究获得当地伦理委员会批准。
纳入64例非感染性儿童葡萄膜炎病例。首次诊断年龄范围为2至17岁,呈双峰分布,52%为男性。前葡萄膜炎是最常见的表现形式,其次是中间葡萄膜炎、后葡萄膜炎和全葡萄膜炎。局部治疗使23%的患者病情缓解,抗代谢药物使12%的患者病情缓解,升级使用肿瘤坏死因子α抑制剂使30%的患者病情缓解。分别有16%和17%的患者采用了替代治疗或仅进行观察。从首次就诊到开始使用抗代谢药物或肿瘤坏死因子α抑制剂的中位时间分别为115天和269天。随访第一年的会诊中位数为8次。随着每次治疗升级,第一年的会诊频率增加。不同治疗组之间的视力结果没有差异。
就视力结果而言,逐步升级的治疗方法显示出安全的特征。甲氨蝶呤呈现出高治疗失败率和不良反应。阿达木单抗和英夫利昔单抗有效且安全。及时的治疗升级可能会减轻患病儿童、其家庭和医疗服务提供者的治疗负担。