Chao Chun R, Cannizzaro Nancy, Hahn Erin E, Shen Ernest, Hsu Chunyi, Ngo-Metzger Quyen, Gould Michael K, Munoz-Plaza Corrine E, Kanter Michael H, Wride Patricia, Ajamian Lena H, Hodeib Melissa, Broder Benjamin I, Curiel Ivette T, Castaneda Alicia, Ong Stephanie K, Tewari Krishnansu, Eskander Ramez N, Tewari Devansu, Mittman Brian S
Department of Research and Evaluation, Kaiser Permanente Southern California, 100 S Los Robles Ave, 2 Floor, Pasadena, CA, 91101, USA.
Department of Health Systems Science, Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena, CA, USA.
Implement Sci. 2025 May 12;20(1):21. doi: 10.1186/s13012-025-01432-9.
Recent updates to national guidelines recommend primary human papillomavirus (HPV) screening for routine cervical cancer screening alongside previously recommended screening options. However, limited guidance exists for implementation approaches that best facilitate cancer screening practice substitution and achieve optimal stakeholder-centered outcomes. We compared "centrally-administered + locally-tailored" (here after referred to as locally-tailored) vs. "centrally-administered + usual care" (here after referred to as centrally-administered) approaches for achieving substitution of HPV and cytology co-testing with primary HPV screening for routine cervical cancer screening to examine the effect of local tailoring on implementation and stakeholder-centered outcomes.
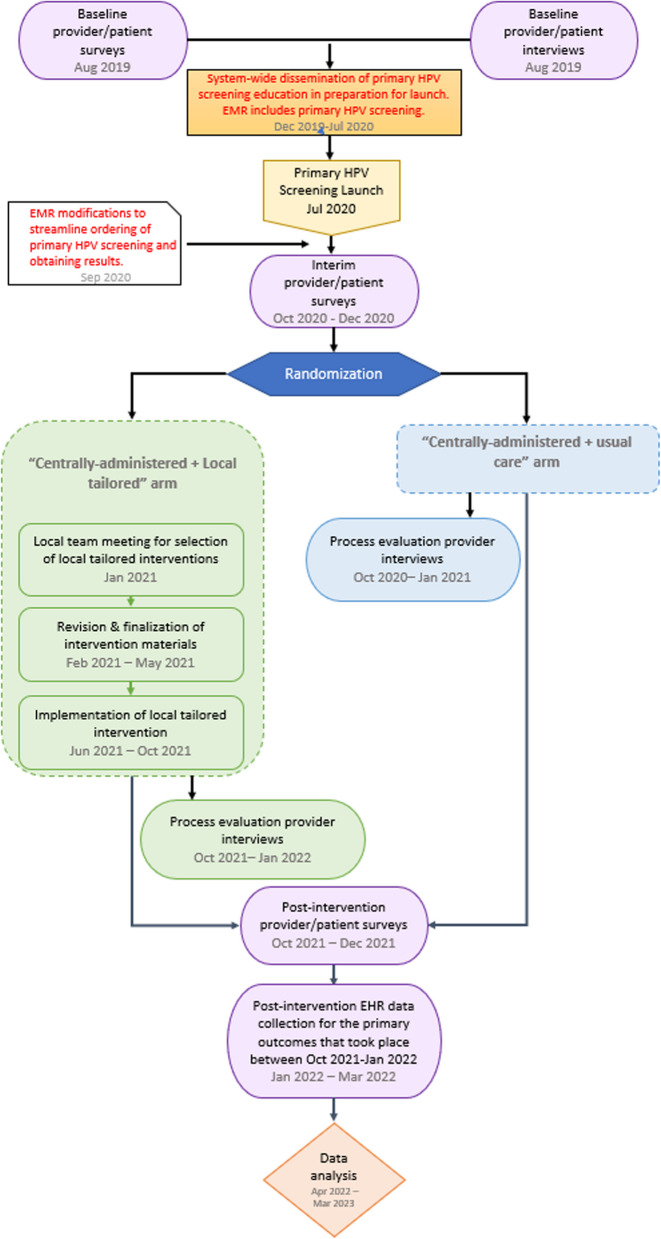
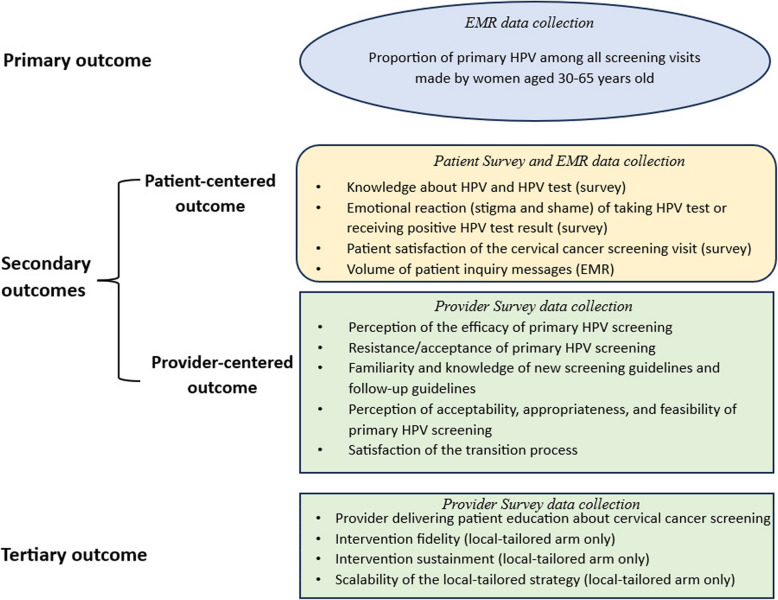
We conducted a pragmatic, cluster randomized trial embedded in the Kaiser Permanente Southern California (KPSC) health system, randomly assigning site groups to study arms at the level of the geographic service area (12 service area randomized). The study took place between 2020-2022. Centrally-administered implementation strategy bundles included physician and staff educational activities. Sites in the locally-tailored arm underwent local needs assessment followed by local selection, tailoring and deployment of implementation strategy bundles. The primary outcome was the proportion of primary HPV screenings among all screenings performed. Secondary stakeholder-centered outcomes included patient (knowledge, emotional reaction, satisfaction, volume of patient inquiries) and provider outcomes (perception, knowledge, acceptance, and satisfaction) measured via repeated surveys or electronic health records. The generalized estimating equation framework and the difference-in-differences approach were used to compare outcomes across study arms.
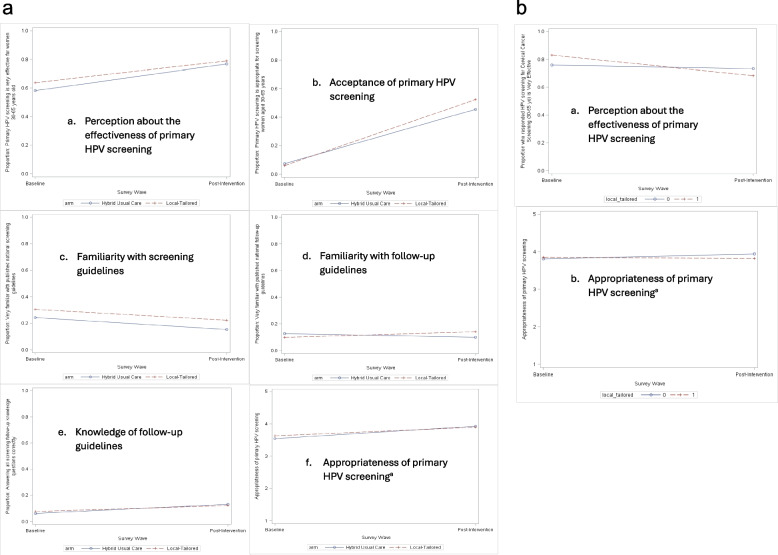
The proportion of appropriate screenings (i.e., use of primary HPV screening) during the post-intervention period was high, with no observed difference between study arms: 98.4% (95% confidence interval [CI] 96.3%-100%) for the locally-tailored arm and 99.1% (95% CI: 97.8%-100%) for the centrally-administered arm (p = 0.34). There were no statistically or clinically significant differences in patient- and provider- outcomes between study arms.
Primary HPV screening was feasible and demonstrated high fidelity in all KPSC service areas. The locally-tailored practice substitution approach and centrally-administered practice substitution approach both achieved near complete uptake of primary HPV screening. Further, similar effects on stakeholder-centered outcomes were observed for both approaches. However, generalizability of our findings may be limited due to unique features of our integrated health system.
NCT04371887. Registered 30 April 2020, URL: https://clinicaltrials.gov/study/NCT04371887?cond=primary%20HPV%20screening&rank=5 .
国家指南的最新更新建议将原发性人乳头瘤病毒(HPV)筛查作为常规宫颈癌筛查的方法,同时保留先前推荐的筛查选项。然而,关于如何以最佳方式促进癌症筛查实践替代并实现以利益相关者为中心的最佳结果的实施方法,指导意见有限。我们比较了“集中管理+因地制宜”(以下简称因地制宜)与“集中管理+常规护理”(以下简称集中管理)两种方法,以实现用原发性HPV筛查替代HPV和细胞学联合检测用于常规宫颈癌筛查,并研究因地制宜对实施情况和以利益相关者为中心的结果的影响。
我们在南加州凯撒医疗集团(KPSC)医疗系统中进行了一项实用的整群随机试验,在地理服务区层面将站点组随机分配到研究组(12个服务区被随机分组)。该研究于2020年至2022年期间进行。集中管理的实施策略包包括医生和工作人员的教育活动。因地制宜组的站点进行了当地需求评估,随后进行了当地选择、因地制宜地制定和部署实施策略包。主要结果是在所有进行的筛查中,原发性HPV筛查的比例。以利益相关者为中心的次要结果包括通过重复调查或电子健康记录测量的患者结果(知识、情绪反应、满意度、患者咨询量)和提供者结果(认知、知识、接受度和满意度)。使用广义估计方程框架和差异法来比较各研究组的结果。
干预后期适当筛查(即使用原发性HPV筛查)的比例很高,各研究组之间未观察到差异:因地制宜组为98.4%(95%置信区间[CI]96.3%-100%),集中管理组为99.1%(95%CI:97.8%-100%)(p=0.34)。各研究组在患者和提供者结果方面没有统计学或临床显著差异。
原发性HPV筛查在所有KPSC服务区都是可行的,并显示出高保真度。因地制宜的实践替代方法和集中管理的实践替代方法都实现了原发性HPV筛查的近乎完全采用。此外,两种方法对以利益相关者为中心的结果观察到了类似的效果。然而,由于我们综合医疗系统的独特特征,我们研究结果的普遍性可能有限。
NCT04371887。于2020年4月30日注册,网址:https://clinicaltrials.gov/study/NCT04371887?cond=primary%20HPV%20screening&rank=5 。