Sharif Sameer, Flindall Holden, Basmaji John, Ablordeppey Enyo, Díaz-Gómez José L, Lanspa Michael, Nikravan Sara, Piticaru Joshua, Lewis Kimberley
Department of Medicine, Division of Emergency Medicine, McMaster University, Hamilton, ON, Canada.
Department of Medicine, Division of Critical Care, McMaster University, Hamilton, ON, Canada.
Crit Care Explor. 2025 May 14;7(5):e1261. doi: 10.1097/CCE.0000000000001261. eCollection 2025 May 1.
To determine the safety and efficacy of critical care ultrasonography (CCUS) guided volume management in acutely ill patients.
We searched MEDLINE, Embase, Wiley CENTRAL, and unpublished sources from inception to February 6, 2024.
We included randomized controlled trials (RCTs) of acutely ill adult patients randomized to receive CCUS as compared with no CCUS to guide fluid management.
Reviewers screened abstracts, full texts, and extracted data independently and in duplicate. We pooled data using a random-effects model, assessed the risk of bias using the modified Cochrane tool and assessed the certainty of evidence using the Grading Recommendations Assessment, Development, and Evaluation approach.
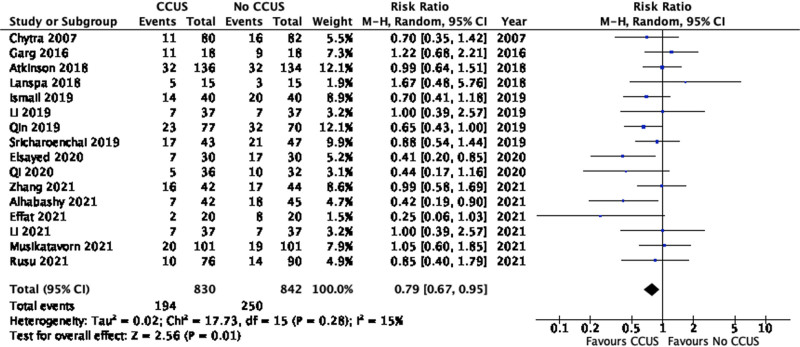
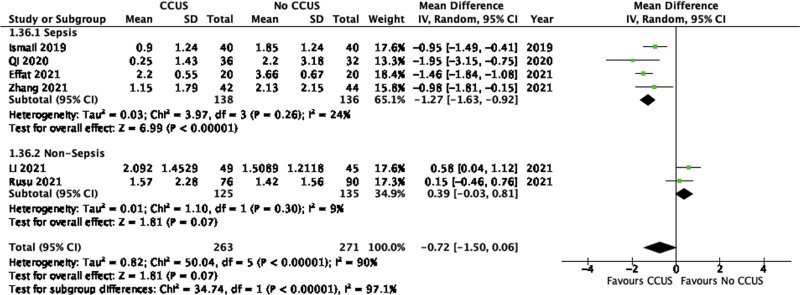
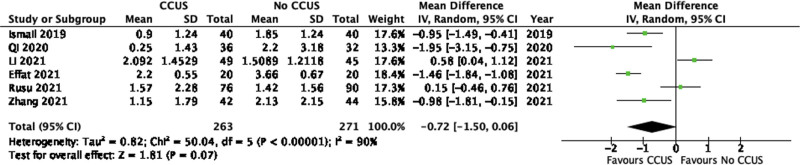
We included 17 RCTs (n = 1765 patients) in this review. Pooled analyses found that the use of CCUS for volume management in acutely ill patients may decrease mortality at the longest reported time period (relative risk [RR], 0.79; 95% CI, 0.67-0.95; low certainty) and decreases the fluid balance up to 72 hours after admission (mean difference [MD], 0.72 L lower; 95% CI, 1.5 L lower to 0.07 L higher; low certainty). CCUS had an uncertain effect on duration of mechanical ventilation (MD, 1.14 d fewer; 95% CI, 3.35 d fewer to 1.07 d more; very low certainty), ICU length of stay (LOS) (MD, 0.01 d fewer; 95% CI, 1.12 d fewer to 1.09 d more; very low certainty), the need for vasopressors (RR, 0.39; 95% CI, 0.10-1.62; very low certainty), acute kidney injury (AKI) (RR, 0.94; 95% CI, 0.32-2.72; very low certainty), and the need for renal replacement therapy (RRT) (RR, 0.79; 95% CI, 0.17-3.66; very low certainty).
In acutely ill adult patients, CCUS for the use of targeted volume management may reduce mortality and fluid balance up to 72 hours after admission. CCUS has an uncertain effect on ICU LOS, duration of mechanical ventilation, duration of vasopressor use, AKI, and the need for RRT. However, this evidence is limited by imprecision and indirectness.
确定重症超声检查(CCUS)引导的容量管理在急性病患者中的安全性和有效性。
我们检索了MEDLINE、Embase、Wiley CENTRAL以及从创刊至2024年2月6日的未发表资料。
我们纳入了将急性病成年患者随机分为接受CCUS或不接受CCUS以指导液体管理的随机对照试验(RCT)。
评审员独立且重复地筛选摘要、全文并提取数据。我们使用随机效应模型汇总数据,使用改良的Cochrane工具评估偏倚风险,并使用分级推荐评估、发展和评价方法评估证据的确定性。
本综述纳入了17项RCT(n = 1765例患者)。汇总分析发现,在急性病患者中使用CCUS进行容量管理可能会在最长报告时间段降低死亡率(相对风险[RR],0.79;95%置信区间[CI],0.67 - 0.95;低确定性),并在入院后72小时内降低液体平衡(平均差[MD],低0.72L;95%CI,低1.5L至高0.07L;低确定性)。CCUS对机械通气时间(MD,少1.14天;95%CI,少3.35天至多1.07天;极低确定性)、重症监护病房(ICU)住院时间(LOS)(MD,少0.01天;95%CI,少1.12天至多1.09天;极低确定性)、血管活性药物使用需求(RR,0.39;95%CI,0.10 - 1.62;极低确定性)、急性肾损伤(AKI)(RR,0.94;95%CI,0.32 - 2.72;极低确定性)以及肾脏替代治疗(RRT)需求(RR,0.79;95%CI,0.17 - 3.66;极低确定性)的影响不确定。
在急性病成年患者中,使用CCUS进行目标容量管理可能会降低死亡率并在入院后72小时内改善液体平衡。CCUS对ICU LOS、机械通气时间、血管活性药物使用时间、AKI以及RRT需求的影响不确定。然而,该证据受精确性和间接性的限制。