Madugalle Thennakoon Mudiyanselage Salila Sameera Bandara, Jayasundara Dissanayaka Mudiyanselage Chandana Sirimewan, Jayawardane Indu Asanka
Teaching Hospital Peradeniya, Kandy, Sri Lanka.
Department of Obstetrics and Gynecology, Faculty of Medicine, University of Colombo, Colombo, Sri Lanka.
PLoS One. 2025 May 20;20(5):e0324172. doi: 10.1371/journal.pone.0324172. eCollection 2025.
Any intervention aimed at maximizing the spontaneous onset of labor and preventing formal induction will be beneficial to the client and welcomed by the provider, because it reduces postmaturity and formal labour induction.
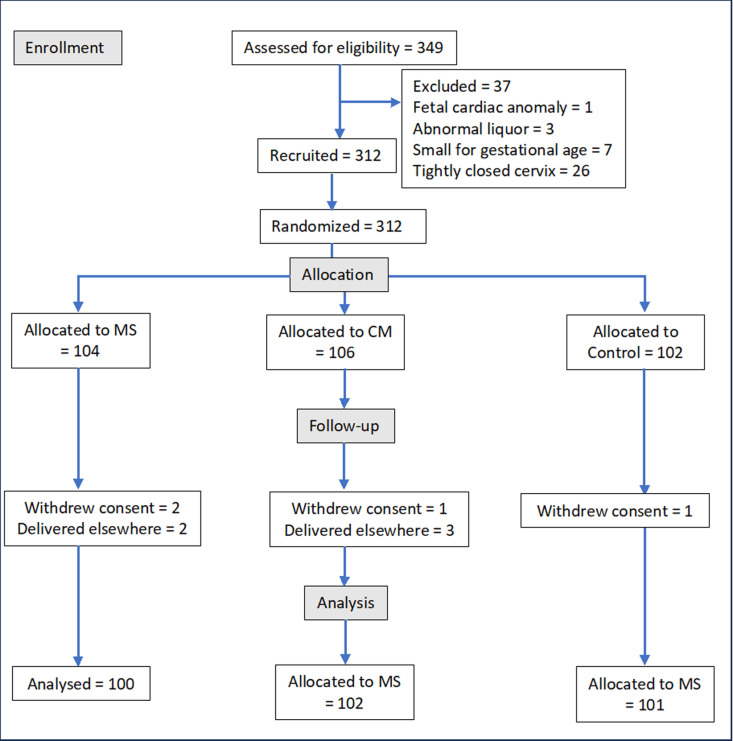
We recruited and randomized 312 uncomplicated singleton pregnancies at 38 weeks of gestation into three groups: membrane sweep (MS), cervical massage (CM), and sham sweep (control). Each intervention was administered at 39 weeks and repeated at 40 weeks of gestation if spontaneous labor, defined as a Modified Bishop's Score of ≥7, did not occur. (Sri Lanka clinical trials registry - SLCTR/2020/003).
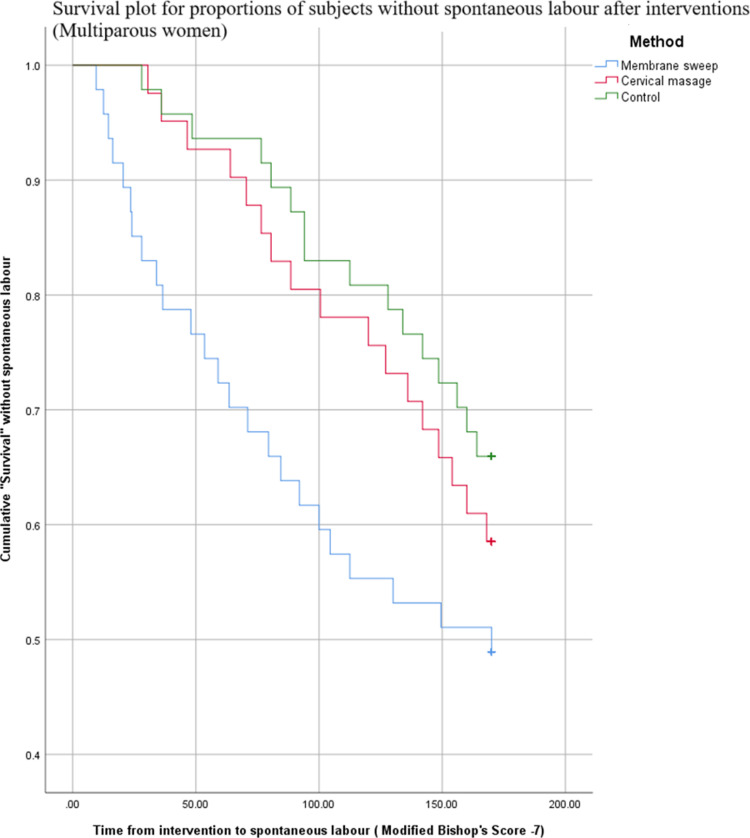
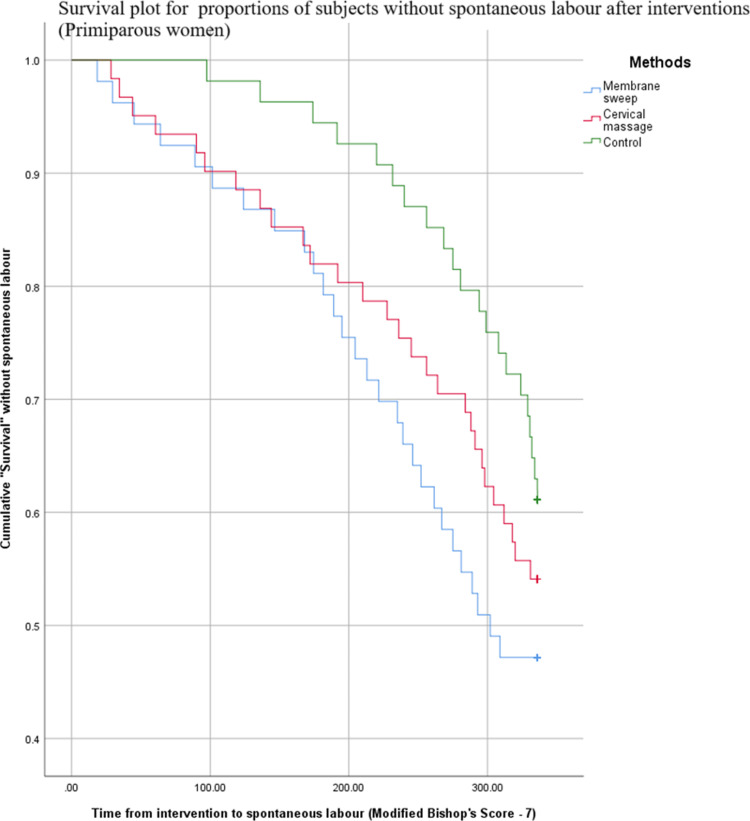
The membrane sweep reduced the need for formal induction, whereas cervical massage did not. (MS vs C RR = 1.4195, 95% CI = 1.0326-1.9513, p = 0.0310; MS vs C OR=1.8739, 95% CI = 1.0664-3.2927, p = 0.0290; Number Needed to Treat = 7; CM vs C RR = 1.2043, 95% CI = 0.8598-1.6867, p = 0.2795). "Survival without spontaneous labor," was lower after the membrane sweep than in controls overall (MS vs C - p = 0.007; CM vs C - p = 0.261), among primiparous (MS vs C p = 0.047; CM vs C p = 0.269) and multiparous (MS vs C p = 0.038; CM vs C p = 0.456) women. The membrane sweep and cervical massage were safe concerning feto-maternal complications and both reduced hospital-stay duration among multiparous women (MS vs C p < 0.0001, 95% CI = 0.5293-1.1791; CM vs C p < 0.0001, 95% CI = 0.6816-1.3552). There was no increased risk of emergency cesarean delivery, oxytocin augmentation, uterine hyperstimulation, postpartum bleeding, maternal pyrexia, or Apgar score < 7 at 5 minutes (p > 0.05). The membrane sweep was less acceptable compared to cervical massage, regardless of parity (MS vs C Primi p = 0.001, Multi p = 0.0216).
We recommend routine offer of membrane sweep to reduce the need for formal induction in term uncomplicated pregnancies, but clinicians should be aware of its inherent discomfort to women.
任何旨在最大程度地促使自然发动分娩并避免正式引产的干预措施,都将对产妇有益且受到医护人员的欢迎,因为这可减少过期产和正式引产的情况。
我们招募了312例妊娠38周的无并发症单胎孕妇,并将其随机分为三组:人工破膜(MS)组、宫颈按摩(CM)组和假破膜(对照组)。每种干预措施均在妊娠39周时进行,若未出现定义为改良Bishop评分≥7的自然分娩,则在妊娠40周时重复进行。(斯里兰卡临床试验注册中心 - SLCTR/2020/003)。
人工破膜减少了正式引产的需求,而宫颈按摩则没有。(MS组与对照组相比,相对危险度(RR)=1.4195,95%置信区间(CI)=1.0326 - 1.9513,p = 0.0310;MS组与对照组相比,比值比(OR)=1.8739,95%CI = 1.0664 - 3.2927,p = 0.0290;需治疗人数(NNT)=7;CM组与对照组相比,RR = 1.2043,95%CI = 0.8598 - 1.6867,p = 0.2795)。总体而言,人工破膜后“未自然分娩的存活情况”低于对照组(MS组与对照组相比 - p = 0.007;CM组与对照组相比 - p = 0.261),初产妇(MS组与对照组相比,p = 0.047;CM组与对照组相比,p = 0.269)和经产妇(MS组与对照组相比,p = 0.038;CM组与对照组相比,p = 0.456)中也是如此。人工破膜和宫颈按摩在母婴并发症方面是安全的,并且都缩短了经产妇的住院时间(MS组与对照组相比,p < 0.0001,95%CI = 0.5293 - 1.1791;CM组与对照组相比,p < 0.0001,95%CI = 0.6816 - 1.3552)。紧急剖宫产、催产素加强宫缩、子宫过度刺激、产后出血、产妇发热或5分钟时阿氏评分<7的风险均未增加(p > 0.05)。无论产妇胎次如何,人工破膜与宫颈按摩相比,接受度较低(初产妇中MS组与对照组相比,p = 0.001;经产妇中MS组与对照组相比,p = 0.0216)。
我们建议对足月无并发症妊娠常规进行人工破膜,以减少正式引产的需求,但临床医生应意识到其给女性带来的固有不适。