Chiu Michael H, Dong Yuan, Fine Nowell, McAlister Finlay A, Sajobi Tolulope, Southern Danielle A, Youngson Erik, van Diepen Sean, James Matthew T, Wilton Stephen B
Libin Cardiovascular Institute, Department of Cardiac Sciences University of Calgary, Calgary, Alberta, Canada; Department of Critical Care Medicine, University of Calgary, Calgary, Alberta, Canada.
Alberta Strategy for Patient Oriented Research Support Unit, Edmonton, Alberta, Canada; Data and Analytics, Alberta Health Services, Alberta, Canada.
JACC Adv. 2025 May 22;4(6 Pt 1):101814. doi: 10.1016/j.jacadv.2025.101814.
The role of routine beta-blocker (BB) use after uncomplicated acute myocardial infarction (AMI) treated with contemporary therapies is not well established.
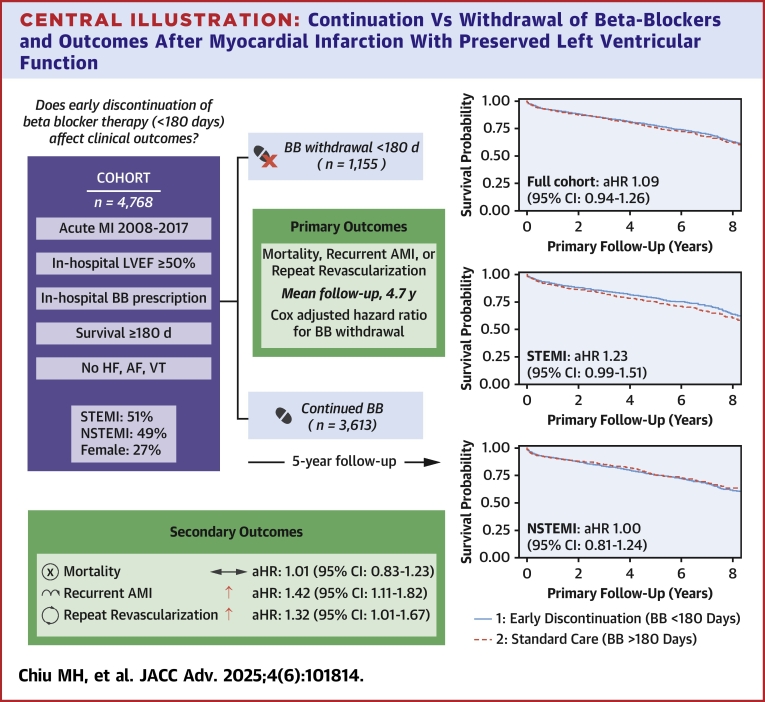
The authors conducted a retrospective cohort study using linked registry and administrative data to evaluate whether early BB discontinuation (a prescription ending within 180 days of discharge) is associated with clinical outcomes.
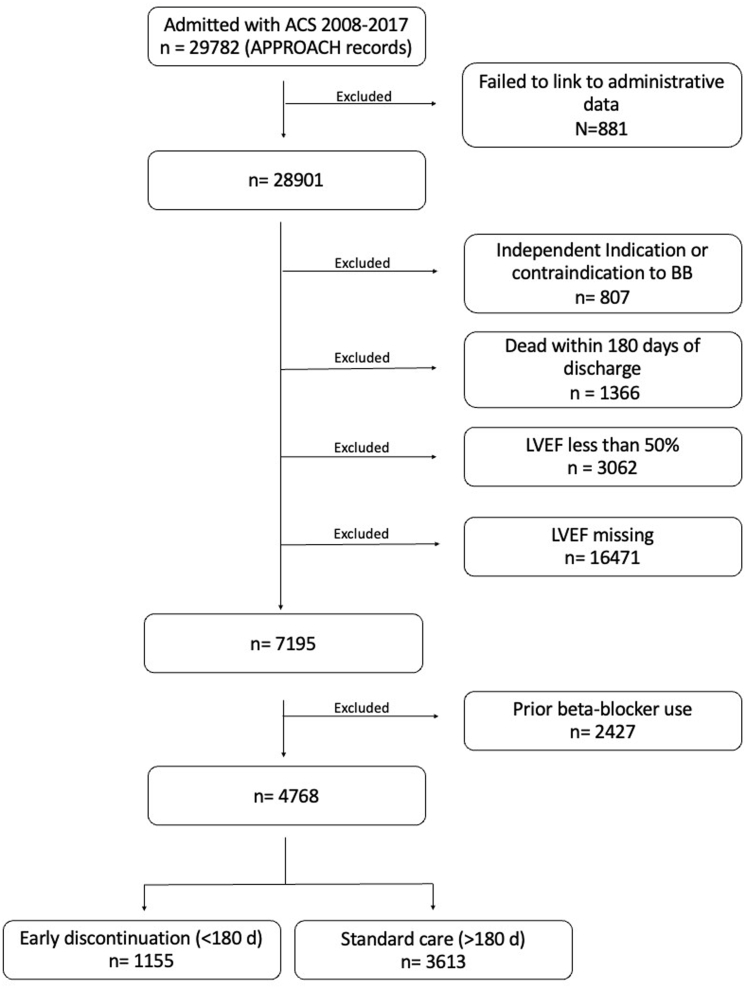
We included patients who survived at least 180 days after AMI from 2008 to 2017 with new BB prescription and left ventricular ejection fraction ≥50%. The primary outcome was a composite of recurrent AMI, myocardial revascularization, or all-cause mortality within 5 years. Secondary outcomes were each of the components of the composite. Cox proportional hazard models were used to evaluate the association between early BB discontinuation and outcomes.
Among the 4,768 included patients, 1,155 (24.2%) discontinued BB within 180 days of AMI discharge. During a median follow-up time of 57 months, 964 patients (20.2%) experienced the primary outcome. Early BB discontinuation was not associated with an increased risk of the primary outcome (adjusted HR: 1.09; 95% CI: 0.94-1.26), or with all-cause mortality (HR: 1.04; 95% CI: 0.86-1.26). However, early BB discontinuation was associated with an increased risk for recurrent AMI and a higher rate of repeat revascularization.
In patients with preserved left ventricular ejection fraction after AMI, discontinuation of BB within 180 days was not associated with a significantly increased risk of a composite outcome of death, recurrent AMI, or revascularization but was associated with increased risk of recurrent AMI and need for repeat revascularization.
在采用当代疗法治疗的无并发症急性心肌梗死(AMI)后常规使用β受体阻滞剂(BB)的作用尚未明确。
作者进行了一项回顾性队列研究,利用关联的登记和管理数据来评估早期停用BB(出院后180天内处方结束)是否与临床结局相关。
我们纳入了2008年至2017年AMI后存活至少180天、有新的BB处方且左心室射血分数≥50%的患者。主要结局是5年内复发性AMI、心肌血运重建或全因死亡的复合结局。次要结局是该复合结局的各个组成部分。采用Cox比例风险模型评估早期停用BB与结局之间的关联。
在纳入的4768例患者中,1155例(24.2%)在AMI出院后180天内停用了BB。在中位随访时间57个月期间,964例患者(20.2%)发生了主要结局。早期停用BB与主要结局风险增加无关(调整后HR:1.09;95%CI:0.94 - 1.26),也与全因死亡无关(HR:1.04;95%CI:0.86 - 1.26)。然而,早期停用BB与复发性AMI风险增加及重复血运重建率较高相关。
在AMI后左心室射血分数保留的患者中,180天内停用BB与死亡、复发性AMI或血运重建的复合结局风险显著增加无关,但与复发性AMI风险增加及重复血运重建需求相关。