Lonergan Bradley, Seemungal Barry M, Ciocca Matteo, Tai Yen F
Department of Brain Sciences, Imperial College London, London W6 8RF, UK.
Department of Neurology, Charing Cross Hospital, Imperial College Healthcare Trust (ICHT), London W2 1NY, UK.
Brain Sci. 2025 May 21;15(5):535. doi: 10.3390/brainsci15050535.
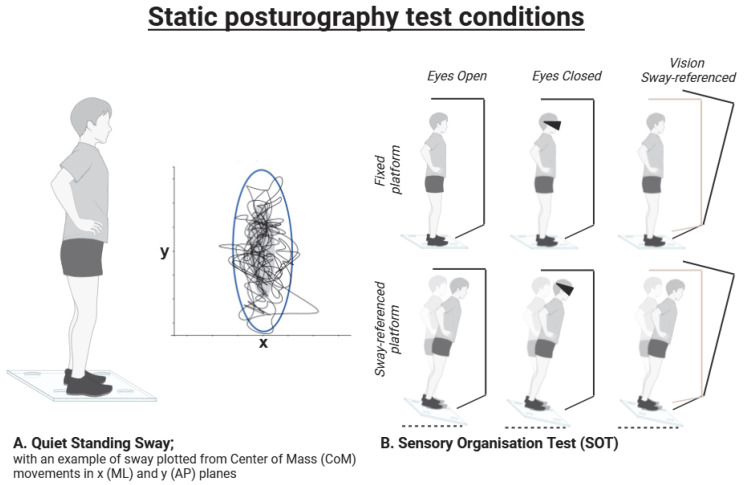
Postural imbalance with falls affects 80% of patients with Parkinson's disease (PD) at 10 years. Standard PD therapies (e.g., levodopa and/or deep brain stimulation-DBS) are poor at improving postural imbalance. Additionally, the mechanistic complexity of interpreting postural control is a major barrier to improving our understanding of treatment effects. In this paper, we review the effects of DBS on balance as measured using posturography. We also critically appraise the quantitative measures and analyses used in these studies.
A literature search was performed independently by 2 researchers using the PUBMED database. Thirty-eight studies are included in this review, with DBS at the subthalamic nucleus (STN-) ( = 25), globus pallidus internus (GPi-) ( = 6), ventral intermediate nucleus (VIM)/thalamus ( = 2), and pedunculopontine nucleus (PPN) ( = 5).
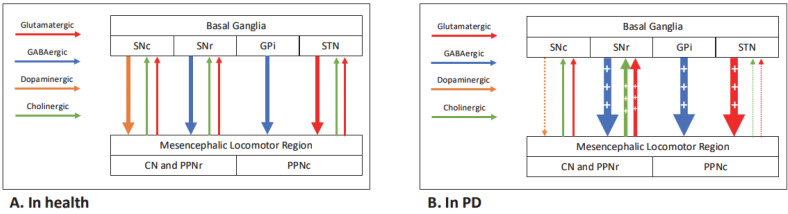
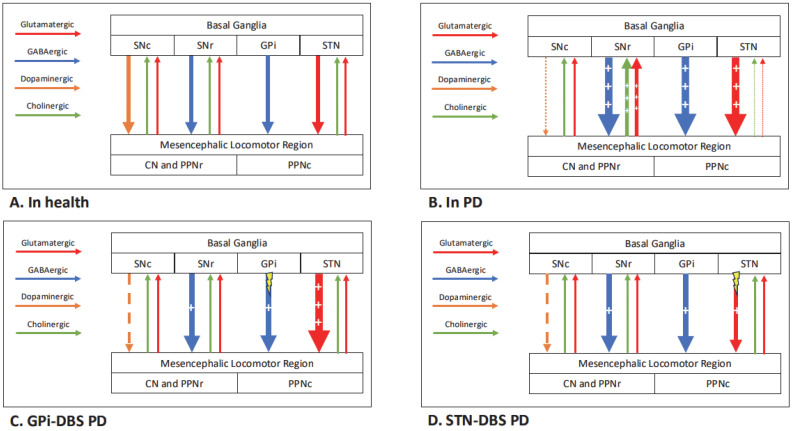
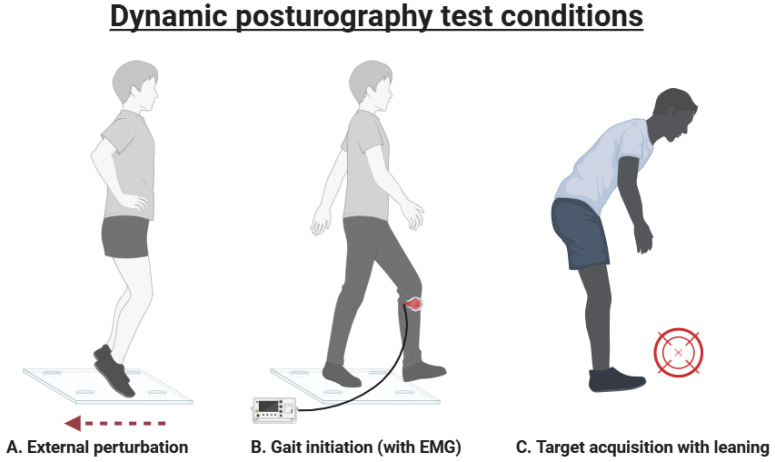
STN- and GPi-DBS reduce static sway in PD and mitigate the increased sway from levodopa. STN-DBS impairs automatic responses to perturbations, whilst GPi-DBS has a more neutral effect. STN-DBS may promote protective strategies following external perturbations but does not improve adaptation. The evidence regarding the effects on gait initiation is less clear. Insufficient evidence exists to make conclusions regarding VIM- and PPN-DBS.
STN- and GPi-DBS have differing effects on posturography, which suggests site-specific and possibly non-dopaminergic mechanisms. Posturography tests should be utilised to answer specific questions regarding the mechanisms of and effects on postural control following DBS. We recommend standardising posturography measures and test conditions by expert consensus and greater long-term data collection, utilising ongoing DBS registries.
姿势失衡伴跌倒在帕金森病(PD)患者病程10年时影响80%的患者。标准的PD治疗方法(如左旋多巴和/或脑深部电刺激-DBS)在改善姿势失衡方面效果不佳。此外,解释姿势控制的机制复杂性是增进我们对治疗效果理解的主要障碍。在本文中,我们回顾了使用姿势描记法测量的DBS对平衡的影响。我们还对这些研究中使用的定量测量和分析进行了批判性评价。
两名研究人员独立使用PUBMED数据库进行文献检索。本综述纳入了38项研究,其中丘脑底核(STN-)DBS(n = 25)、内侧苍白球(GPi-)DBS(n = 6)、腹中间核(VIM)/丘脑DBS(n = 2)和脚桥核(PPN)DBS(n = 5)。
STN-和GPi-DBS可减少PD患者的静态摇摆,并减轻左旋多巴引起的摇摆增加。STN-DBS会损害对扰动的自动反应,而GPi-DBS的影响更为中性。STN-DBS可能会促进外部扰动后的保护性策略,但不会改善适应性。关于对步态起始影响的证据尚不清楚。没有足够的证据就VIM-和PPN-DBS得出结论。
STN-和GPi-DBS对姿势描记法有不同影响,这表明存在部位特异性且可能是非多巴胺能机制。应利用姿势描记法测试来回答有关DBS后姿势控制机制及影响的具体问题。我们建议通过专家共识使姿势描记法测量和测试条件标准化,并利用正在进行的DBS注册库收集更多长期数据。