Rosati Fabrizio, Baudo Massimo, Di Bacco Lorenzo, Oosterlinck Wouter, Torregrossa Gianluca, Tomasi Cesare, Boldini Francesca, Muneretto Claudio, Benussi Stefano
Division of Cardiac Surgery, ASST Spedali Civili Di Brescia, University of Brescia, P.Le Spedali Civili, 1, 25123, Brescia, Italy.
Department of Cardiac Surgery Research, Lankenau Institute for Medical Research, Main Line Health, Wynnewood, PA, USA.
J Robot Surg. 2025 May 28;19(1):245. doi: 10.1007/s11701-025-02370-w.
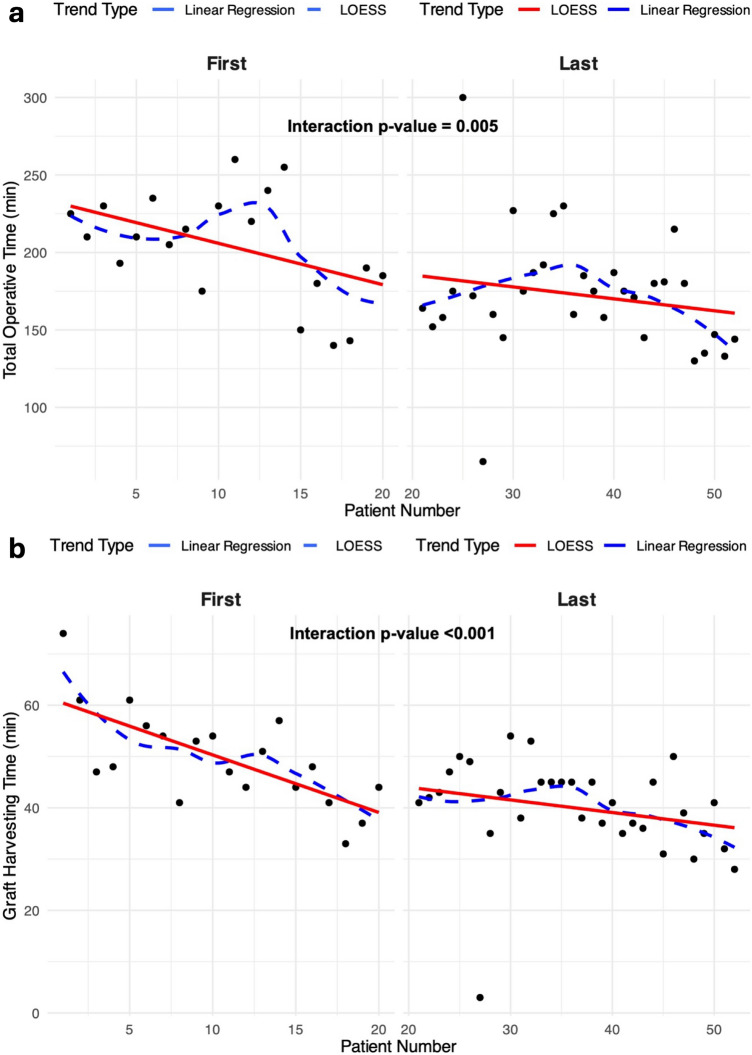
Adoption of robot-assisted coronary artery bypass grafting (RA-MIDCAB) remains limited due to concerns about learning curves, outcomes, and patient-specific anatomic challenges. This study evaluates our initial single-center experience with RA-MIDCAB. Between December 2022 and June 2024, 52 patients underwent RA-MIDCAB. Inclusion criteria comprised isolated left anterior descending artery (LAD) stenosis or LAD revascularization as part of a hybrid valvular/coronary strategy. Primary endpoints were 30-day mortality, conversion to sternotomy, and graft injury. Operative times and biometric indices (body indices such as body mass index [BMI], Haller Index, and Cardiothoracic Ratio) were analyzed for correlation with learning curve progression and surgical outcomes. Mean age was 68.5 ± 11.5 years, and 82.7% (43/52) were males. Robotic LITA harvesting was successfully completed in 98.1% (51/52) of patients (one patient had a graft injury), with no perioperative mortality. Postoperative complications occurred in 38.5% (20/52), mostly due to atrial fibrillation (19.2%, 10/52) and acute kidney injury (13.5%, 7/52) with no correlation with operative times at logistic regression. According to thoracic indexes, no correlation was found between chest complexity and postoperative complications. Neither EuroSCORE II, BMI nor thoracic indices significantly impacted operative times. Linear regression demonstrated significant reductions in overall surgical and graft-harvesting times across the experience, suggesting improved efficiency. RA-MIDCAB is feasible and safe, even in patients with challenging thoracic anatomy. This early experience demonstrated promising outcomes and significant learning curve improvements, supporting the potential for broader adoption of this technique even in patients unlikely deemed suitable for minimally invasive cardiac revascularization surgery.
由于对学习曲线、手术结果以及患者特定解剖结构挑战的担忧,机器人辅助冠状动脉搭桥术(RA-MIDCAB)的采用率仍然有限。本研究评估了我们在单中心开展RA-MIDCAB的初步经验。在2022年12月至2024年6月期间,52例患者接受了RA-MIDCAB手术。纳入标准包括孤立的左前降支(LAD)狭窄或作为瓣膜/冠状动脉杂交策略一部分的LAD血运重建。主要终点为30天死亡率、转为开胸手术以及移植血管损伤。分析手术时间和生物测量指标(如体重指数[BMI]、哈勒指数和心胸比率等身体指标)与学习曲线进展和手术结果的相关性。平均年龄为68.5±11.5岁,82.7%(43/52)为男性。98.1%(51/52)的患者成功完成了机器人内乳动脉采集(1例患者发生移植血管损伤),无围手术期死亡。38.5%(20/52)的患者出现术后并发症,主要原因是心房颤动(19.2%,10/52)和急性肾损伤(13.5%,7/52),逻辑回归分析显示与手术时间无关。根据胸部指标,未发现胸部复杂程度与术后并发症之间存在相关性。欧洲心脏手术风险评估系统II(EuroSCORE II)、BMI和胸部指标均未对手术时间产生显著影响。线性回归表明,在整个经验过程中,总体手术时间和移植血管采集时间显著缩短,提示效率有所提高。RA-MIDCAB是可行且安全的,即使对于胸部解剖结构具有挑战性的患者也是如此。这一早期经验显示出了良好的结果和显著的学习曲线改善,支持了即使在不太可能被认为适合微创心脏血运重建手术的患者中更广泛采用该技术的潜力。