Rollins Caitlin K, Wypij David, Zambrano Laura D, Calderon Johanna, Taylor Alex M, Worhach Jennifer, Rodriguez Susan, Licht Paul A, Maiman Moshe, Hart Nicholas, Son Mary Beth F, Kossowsky Joe, Friedman Matthew L, Hobbs Charlotte V, Kong Michele, Maddux Aline B, McGuire Jennifer L, Staat Mary Allen, Yonker Lael M, Mazumdar Maitreyi, Newburger Jane W, Randolph Adrienne G, Campbell Angela P
Department of Neurology, Boston Children's Hospital, Boston, Massachusetts.
Department of Neurology, Harvard Medical School, Boston, Massachusetts.
JAMA Netw Open. 2025 Jun 2;8(6):e2512487. doi: 10.1001/jamanetworkopen.2025.12487.
Neurologic and psychological sequelae are observed 1 year after hospitalization for multisystem inflammatory syndrome in children (MIS-C), but whether these concerns persist is not known.
To examine the trajectory of neurologic, psychological, and quality-of-life sequelae up to 2 years after MIS-C.
DESIGN, SETTING, AND PARTICIPANTS: This longitudinal cohort study assessed children diagnosed with MIS-C from August 1, 2020, to August 31, 2021, and matched sibling and community controls, when available. The study was conducted 6 to 12 months and 18 to 24 months after discharge from a US or Canadian hospital. Data analysis was performed from May 2024 to January 2025.
Hospitalization for MIS-C.
A central study site remotely administered a structured interview, surveys, neuropsychological assessment, and neurologic examination. Group differences were assessed using generalized estimating equations, accounting for matching. Variables extracted from hospital records included intensive care unit admission and echocardiographic left ventricular ejection fraction (LVEF).
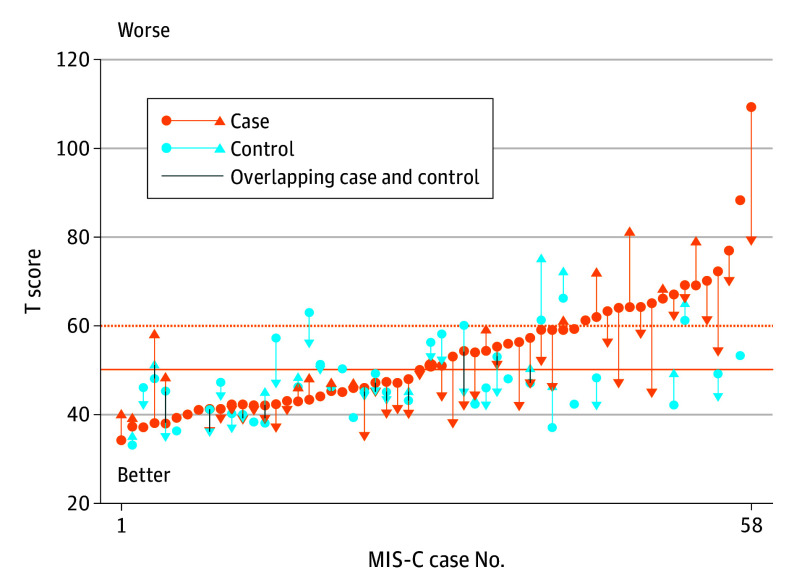
Overall, 95 participants were included in the study; 93 of 108 participants (86%) returned from the year 1 study and 2 participants were added in year 2 (median [IQR] age, 12.6 [11.0-15.7] years; 38 [40%] female and 57 [60%] male). Fifty-nine patients with MIS-C (mean [SD] age, 13.2 [4.0] years; 39 [66%] male) and 36 controls (mean [SD] age, 13.5 [3.5] years; 18 [50%] male) enrolled. In year 2, the MIS-C group was similar to controls on all outcome measures, except they had more somatization symptoms (Behavior Assessment Scale for Children, Third Edition mean [SD] somatization score, 52.1 [13.0] vs 46.5 [8.5]; mean difference, 5.2; 95% CI, 1.3-9.1). Within the MIS-C group, scores generally improved between initial and follow-up evaluations, a finding that was not observed in controls. Eight of 13 children with MIS-C (62%) who had abnormal neurologic examination findings in year 1 had normal examination findings by year 2. Among patients with MIS-C, measures of higher illness severity during hospitalization were associated with worse executive function in year 2 (National Institutes of Health [NIH] List Sort Working Memory Test score, -7.3 points per intensive care unit admission vs not [95% CI, -14.3 to -0.3 points] and -5.8 points per LVEF category change [95% CI, -9.1 to -2.6 points]; verbal fluency switching score, -0.8 points per LVEF category change [95% CI, -1.5 to -0.1 points]).
In this longitudinal, matched cohort study of children with MIS-C and controls followed up sequentially up to 2 years after hospital discharge, children with MIS-C had more somatic symptoms than control children. Overall, however, patients with MIS-C had improved neurologic and psychological outcomes between the testing intervals, performing similarly to controls on most measures by year 2 follow-up. These findings suggest that these concerns may improve over time.
儿童多系统炎症综合征(MIS-C)住院1年后可观察到神经和心理后遗症,但这些问题是否持续存在尚不清楚。
研究MIS-C后长达2年的神经、心理和生活质量后遗症轨迹。
设计、背景和参与者:这项纵向队列研究评估了2020年8月1日至2021年8月31日期间被诊断为MIS-C的儿童,以及匹配的同胞和社区对照(如有)。该研究在从美国或加拿大医院出院后的6至12个月以及18至24个月进行。数据分析于2024年5月至2025年1月进行。
MIS-C住院治疗。
一个中心研究地点远程进行结构化访谈、调查、神经心理评估和神经检查。使用广义估计方程评估组间差异,并考虑匹配因素。从医院记录中提取的变量包括重症监护病房入院情况和超声心动图左心室射血分数(LVEF)。
总体而言,95名参与者纳入研究;108名参与者中的93名(86%)从第1年的研究中返回,第2年增加了2名参与者(年龄中位数[四分位间距],12.6[11.0 - 15.7]岁;38名[40%]女性和57名[60%]男性)。59例MIS-C患者(平均[标准差]年龄,13.2[4.0]岁;39名[66%]男性)和36名对照(平均[标准差]年龄,13.5[3.5]岁;18名[50%]男性)入组。在第2年,MIS-C组在所有结局指标上与对照组相似,但他们有更多的躯体化症状(儿童行为评估量表第三版平均[标准差]躯体化得分,52.1[13.0]对46.5[8.5];平均差异,5.2;95%置信区间,1.3 - 9.1)。在MIS-C组内,分数在初始评估和随访评估之间总体有所改善,这一发现未在对照组中观察到。第1年神经检查结果异常的13名MIS-C儿童中有8名(62%)在第2年检查结果正常。在MIS-C患者中,住院期间疾病严重程度较高的指标与第2年较差的执行功能相关(美国国立卫生研究院[NIH]列表排序工作记忆测试得分,每入住一次重症监护病房降低7.3分,与未入住相比[95%置信区间,-14.3至-0.3分],以及每LVEF类别变化降低5.8分[95%置信区间,-9.1至-2.6分];言语流畅性转换得分,每LVEF类别变化降低0.8分[95%置信区间,-1.5至-0.1分])。
在这项对MIS-C儿童及其对照进行的纵向、匹配队列研究中,出院后连续随访长达2年,MIS-C儿童比对照儿童有更多的躯体症状。然而,总体而言,MIS-C患者在测试间隔之间神经和心理结局有所改善,到第2年随访时在大多数指标上与对照组表现相似。这些发现表明这些问题可能会随着时间改善。