Rotteveel Adriënne Henderika, Klein Petrus Paulus Franciscus, Rodriguez Marlous Joyann, Jansen Marleen Elizabeth, Klaassen Meike M
National Institute for Public Health and the Environment, Centre for Public Health, Healthcare and Society, Antonie van Leeuwenhoeklaan 9, Bilthoven, 3721 MA, the Netherlands.
National Institute for Public Health and the Environment, Centre for Health Protection, Antonie van Leeuwenhoeklaan 9, Bilthoven, 3721 MA, the Netherlands.
BMC Health Serv Res. 2025 Jun 2;25(1):783. doi: 10.1186/s12913-025-12948-7.
Previous estimates of potential costs savings from de-implementation of low-value care have been calculated with simple modelling approaches, focused on direct medical costs and did not take substitution into account. Therefore, the aim of this study was to develop and evaluate a modelling approach to calculate a more realistic estimate of societal costs and benefits of de-implementation of low-value care.
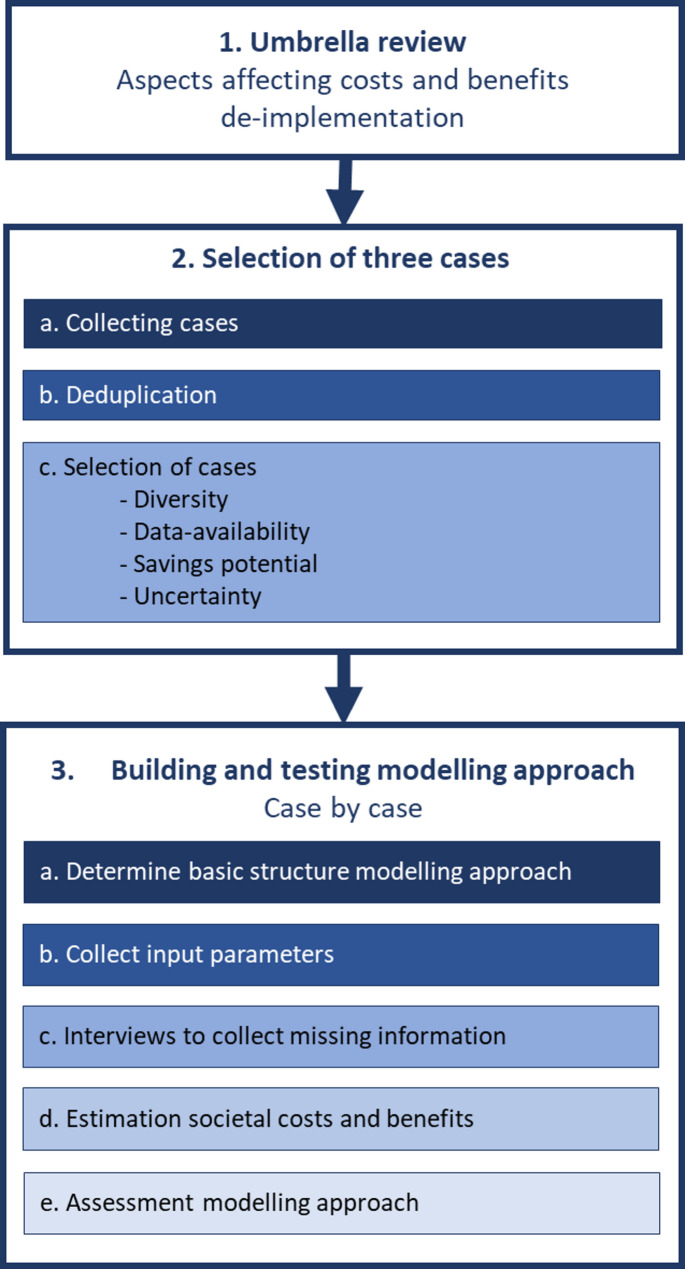
The modelling approach was developed and evaluated in three steps: (1) review of reviews to identify aspects that may affect the costs and benefits of de-implementation, (2) selection of three cases of low-value care, (3) development and evaluation of the modelling approach for each case. Desk research and interviews with actors were used in step 3 to define input parameters.
The modelling approach was build and evaluated for the following cases: (1) surgery for achilles tendon rupture, (2) mammography for women < 30 years with focal breast complaints, and (3) imaging for non-specific low back pain. From the interviews, it appeared that case 2 had already been fully disinvested. Hence, calculating the societal costs and benefits for this case was not considered valuable. For case 1 and 3 it was considered valuable and feasible to calculate the societal costs and benefits. Compared to the adapted societal business case approach used in case 1, the adapted societal cost-benefit analysis approach used for case 3 provided a more realistic and better estimate.
It is feasible to calculate a more elaborate and realistic estimate of societal costs and benefits of the de-implementation of low-value care than previous estimates. Nevertheless, it was not feasible to include the costs of de-implementation itself as these are highly reliant on the specific de-implementation strategy employed, which is context specific. Furthermore, the time needed to calculate a more elaborate and realistic estimate stresses the need to carefully select low-value care cases for which the value of calculating such an elaborate and realistic estimate outweighs the effort required to do so.
The online version contains supplementary material available at 10.1186/s12913-025-12948-7.
先前对取消低价值医疗服务可能节省的潜在成本的估计是通过简单的建模方法计算得出的,这些方法侧重于直接医疗成本,并未考虑替代效应。因此,本研究的目的是开发和评估一种建模方法,以更现实地估计取消低价值医疗服务的社会成本和收益。
建模方法分三步开发和评估:(1)对综述进行回顾,以确定可能影响取消低价值医疗服务成本和收益的因素;(2)选择三个低价值医疗服务案例;(3)针对每个案例开发和评估建模方法。第三步采用案头研究和与相关人员的访谈来确定输入参数。
针对以下案例构建并评估了建模方法:(1)跟腱断裂手术;(2)30岁以下有局灶性乳腺症状女性的乳房X光检查;(3)非特异性下腰痛的影像学检查。从访谈中发现,案例2已完全停止投入。因此,计算该案例的社会成本和收益被认为没有价值。对于案例1和3,计算社会成本和收益被认为是有价值且可行的。与案例1中使用的调整后的社会商业案例方法相比,案例3中使用的调整后的社会成本效益分析方法提供了更现实、更好的估计。
与先前的估计相比,计算取消低价值医疗服务更详尽、现实的社会成本和收益估计是可行的。然而,将取消低价值医疗服务本身的成本纳入计算是不可行的,因为这些成本高度依赖于所采用的具体取消策略,而这是因具体情况而异的。此外,计算更详尽、现实估计所需的时间强调了仔细选择低价值医疗服务案例的必要性,对于这些案例,计算如此详尽、现实估计的价值超过了所需的努力。
在线版本包含可在10.1186/s12913 - 025 - 12948 - 7获取的补充材料。