Kim Dong Geun, Bae Seok Hyun, Kim Dong Ju, Lee Jong Suk, Joo Kwangsic, Park Sang Jun, Woo Se Joon, Park Kyu Hyung
Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Republic of Korea.
Department of Ophthalmology, Seoul National University Bundang Hospital, Seongnam, Republic of Korea.
Ophthalmol Sci. 2025 Apr 1;5(5):100780. doi: 10.1016/j.xops.2025.100780. eCollection 2025 Sep-Oct.
To investigate and compare the clinical characteristics of patients with unilateral high myopia (UHM) and bilateral high myopia (BHM) based on axial length (AL).
A retrospective cohort study.
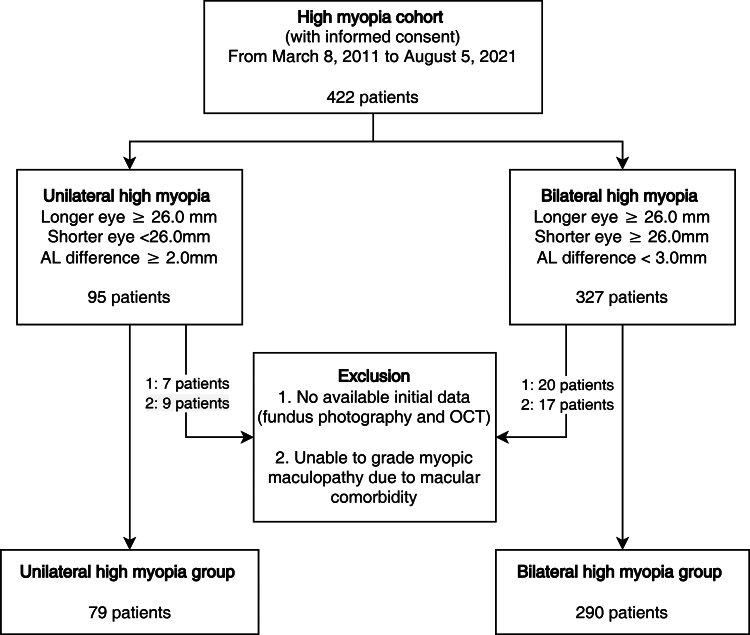
Adult patients diagnosed with UHM or BHM between March 2011 and August 2021.
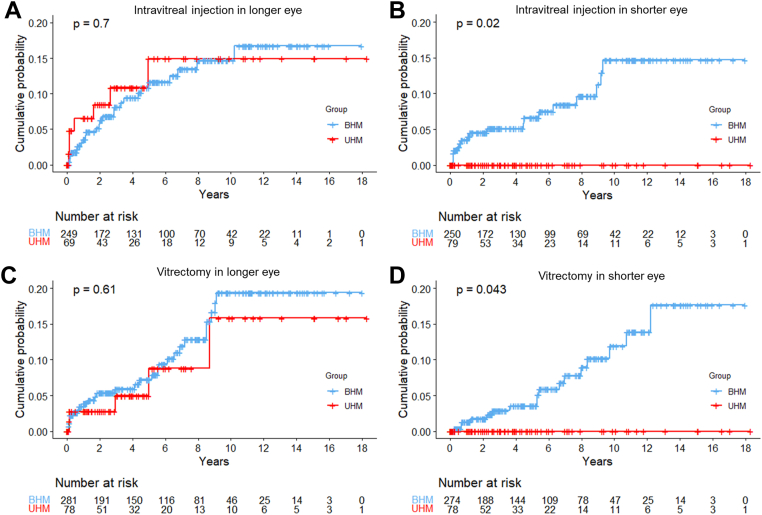
Unilateral high myopia was defined as ≥26 mm AL in 1 eye and <26 mm in the other, with ≥2 mm difference. Bilateral high myopia was defined as ≥26 mm AL in both eyes, with ≤3 mm difference. In each patient, the eye with the longer AL was designated the "longer eye" and the other the "shorter eye." We analyzed differences in clinical features, including ophthalmic history, best-corrected visual acuity, ocular biometry, and myopic maculopathy grade. Myopic maculopathy was graded based on atrophy, traction, and neovascularization using a known method. Long-term features included treatments for myopic neovascular maculopathy and myopic tractional maculopathy and AL change over time.
Comparison of clinical characteristics between UHM and BHM groups.
We analyzed 369 patients (79 with UHM and 290 with BHM) with a median follow-up period of 4.5 years. The UHM group had a higher proportion of women than the BHM group (88.8% vs. 76.2%, = 0.025). Compared with longer eyes in the BHM group, those in the UHM group had worse best-corrected visual acuity (0.8 ± 0.6 vs. 0.6 ± 0.6 in logarithm of the minimum angle of resolution, < 0.001) despite having shorter AL (29.1 ± 1.6 mm vs. 30.6 ± 1.9 mm, < 0.001). In the analysis of AL changes, shorter eyes in the UHM group showed no elongation over time (0.014 mm/year, = 0.12), unlike the longer eyes in UHM and both eyes in BHM (0.049-0.071 mm/year, < 0.01).
Adult UHM patients mostly lacked associated environmental factors. The poorer visual acuity in the longer eyes of UHM patients, which cannot be explained by structural abnormalities, suggests that the interocular difference may have originated in early childhood. During the follow-up period, AL elongation and myopic complications occurred at similar rates in the longer eye of UHM and both eyes of BHM. Meanwhile, such changes were not observed in the shorter eye in UHM. Further investigation of the underlying mechanisms, such as the genetic factors contributing to this extreme asymmetry, is warranted.
The author(s) have no proprietary or commercial interest in any materials discussed in this article.
基于眼轴长度(AL)研究并比较单侧高度近视(UHM)和双侧高度近视(BHM)患者的临床特征。
一项回顾性队列研究。
2011年3月至2021年8月期间诊断为UHM或BHM的成年患者。
单侧高度近视定义为一只眼AL≥26mm,另一只眼<26mm,差值≥2mm。双侧高度近视定义为双眼AL≥26mm,差值≤3mm。在每位患者中,将AL较长的眼指定为“较长眼”,另一只为“较短眼”。我们分析了临床特征的差异,包括眼科病史、最佳矫正视力、眼部生物测量和近视性黄斑病变分级。近视性黄斑病变采用已知方法根据萎缩、牵拉和新生血管进行分级。长期特征包括近视性新生血管性黄斑病变和近视性牵拉性黄斑病变的治疗以及随时间的AL变化。
UHM组和BHM组临床特征的比较。
我们分析了369例患者(79例UHM患者和290例BHM患者),中位随访期为4.5年。UHM组女性比例高于BHM组(88.8%对76.2%,P = 0.025)。与BHM组的较长眼相比,UHM组的较长眼尽管AL较短(29.1±1.6mm对30.6±1.9mm,P<0.001),但最佳矫正视力更差(最小分辨角对数视力为0.8±0.6对0.6±0.6,P<0.001)。在AL变化分析中,UHM组的较短眼随时间未显示伸长(0.014mm/年,P = 0.12),这与UHM组的较长眼和BHM组的双眼不同(0.049 - 0.071mm/年,P<0.01)。
成年UHM患者大多缺乏相关环境因素。UHM患者较长眼较差的视力无法用结构异常解释,提示眼间差异可能始于儿童早期。在随访期间,UHM组较长眼和BHM组双眼的AL伸长和近视并发症发生率相似。同时,UHM组较短眼未观察到此类变化。有必要进一步研究潜在机制,如导致这种极端不对称的遗传因素。
作者对本文讨论的任何材料均无所有权或商业利益。