Tatit Rafael Trindade, Baccin Carlos Eduardo, Nair Priya, Mensah Emmanuel O, Mason James Ryan, Dehkharghani Seena, Copeland Karen, Ogilvy Christopher S
Interventional Neuroradiology, Hospital Israelita Albert Einstein, São Paulo, Brazil.
Department of Biomedical Engineering (2016-2017), Arizona State University, Tempe, United States.
Surg Neurol Int. 2025 May 30;16:213. doi: 10.25259/SNI_1118_2024. eCollection 2025.
Durable occlusion after endovascular coiling can be compromised by recanalization, underscoring the need for accurate cerebral aneurysm assessment. Precise volume measurement not only informs treatment decisions and detects subtle aneurysm growth but also refines calculations of packing density, historically linked to occlusion success. This study compares three volume-measurement approaches-traditional two-dimensional (2D) estimation, a semi-automated three-dimensional (3D) technique, and an artificial intelligence (AI)-based 3D method.
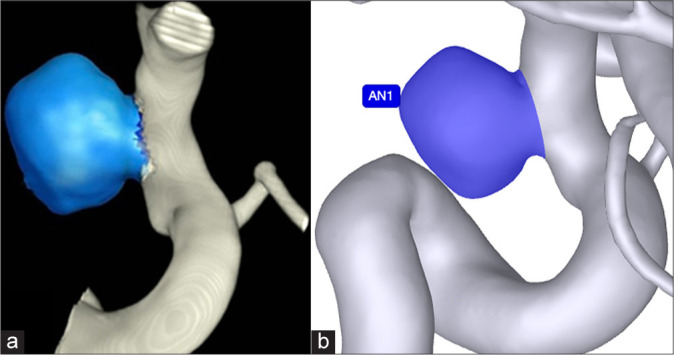
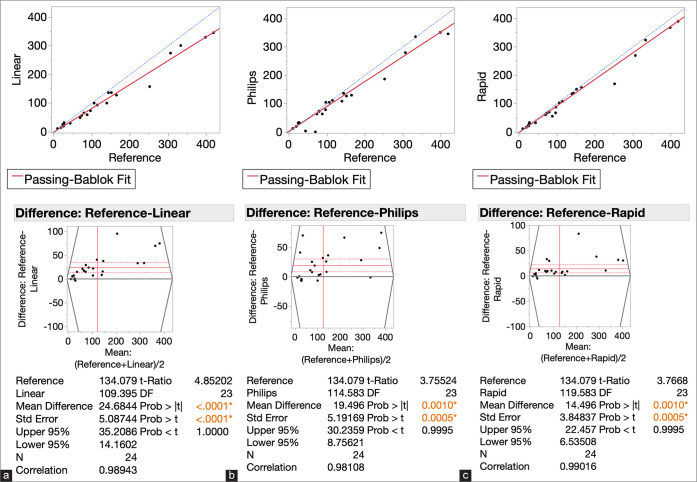
In this retrospective analysis, 24 aneurysms were assessed using 3D rotational angiography. Manual segmentation by three specialists using ITK-SNAP or mimics served as the reference standard. These results were compared with volumes from a semi-automated 3D platform (Philips Advanced Visualization Workspace), an AI-based tool (RapidAI for Aneurysm), and traditional 2D estimations. Agreement with the reference standard was quantified through Passing-Bablok regression slopes and mean biases.
Passing-Bablok slopes for the 2D, Philips, and RapidAI methods were 0.83, 0.87, and 0.94, respectively, while mean biases were -24.7 mm (2D), -19.5 mm (Philips), and -14.5 mm (RapidAI). RapidAI demonstrated the strongest correlation with the reference standard, whereas 2D estimations showed the largest discrepancy. The semi-automated 3D method exhibited intermediate accuracy, potentially influenced by the clinician input required for segmentation.
All methods underestimated aneurysm volumes compared to the reference standard, suggesting that inaccurate volume measurements may mask early aneurysm growth. Among the techniques assessed, the AI-based approach provided the closest agreement with the reference, indicating that improved volumetric methods-particularly AI-driven ones-can enhance early detection of aneurysm expansion, guide treatment decisions, and help establish more reliable follow-up strategies for both treated and conservatively managed aneurysms.
血管内栓塞术后的持久闭塞可能会因再通而受到影响,这突出了准确评估脑动脉瘤的必要性。精确的体积测量不仅有助于治疗决策和检测动脉瘤的细微生长,还能完善填充密度的计算,而填充密度在历史上与闭塞成功率相关。本研究比较了三种体积测量方法——传统的二维(2D)估计法、半自动三维(3D)技术和基于人工智能(AI)的三维方法。
在这项回顾性分析中,使用三维旋转血管造影对24个动脉瘤进行了评估。由三位专家使用ITK-SNAP或mimics进行手动分割作为参考标准。将这些结果与来自半自动三维平台(飞利浦高级可视化工作区)、基于人工智能的工具(用于动脉瘤的RapidAI)和传统二维估计法得出的体积进行比较。通过Passing-Bablok回归斜率和平均偏差对与参考标准的一致性进行量化。
二维、飞利浦和RapidAI方法的Passing-Bablok斜率分别为0.83、0.87和0.94,而平均偏差分别为-24.7毫米(二维)、-19.5毫米(飞利浦)和-14.5毫米(RapidAI)。RapidAI与参考标准的相关性最强,而二维估计法的差异最大。半自动三维方法表现出中等准确性,可能受到分割所需临床医生输入的影响。
与参考标准相比,所有方法均低估了动脉瘤体积,这表明不准确的体积测量可能掩盖动脉瘤的早期生长。在所评估的技术中,基于人工智能的方法与参考标准的一致性最高,这表明改进的体积测量方法——特别是人工智能驱动的方法——可以加强对动脉瘤扩张的早期检测,指导治疗决策,并有助于为已治疗和保守治疗的动脉瘤建立更可靠的随访策略。