Wadhwani Shikha, Mansfield Sarah A, Smith Abigail R, Robinson Bruce M, Abdelghani Eman, Al-Uzri Amira, Ashoor Isa F, Bartosh Sharon M, Chishti Aftab S, Hayek Salim S, Hladunewich Michelle A, Kerlin Bryce A, Madapoosi Siddharth S, Mariani Laura H, Mottl Amy K, Rheault Michelle N, O'Shaughnessy Michelle M, Sperati Christopher John, Srivastava Tarak, Selewski David T, Wang Chia-Shi, Wong Craig S, Weaver Donald J, Khalid Myda
Division of Nephrology and Hypertension, Northwestern Feinberg School of Medicine Chicago, IL.
Arbor Research Collaborative for Health, Ann Arbor, MI.
Kidney Med. 2024 Jul 20;7(6):100877. doi: 10.1016/j.xkme.2024.100877. eCollection 2025 Jun.
RATIONALE & OBJECTIVE: Cardiovascular (CV) and thromboembolic (TE) events are known complications of glomerular disease (GD), but their incidence and risk factors are poorly characterized. This analysis describes CV and TE outcomes in the Cure GlomeruloNephropathy (CureGN) Network.
Prospective cohort study.
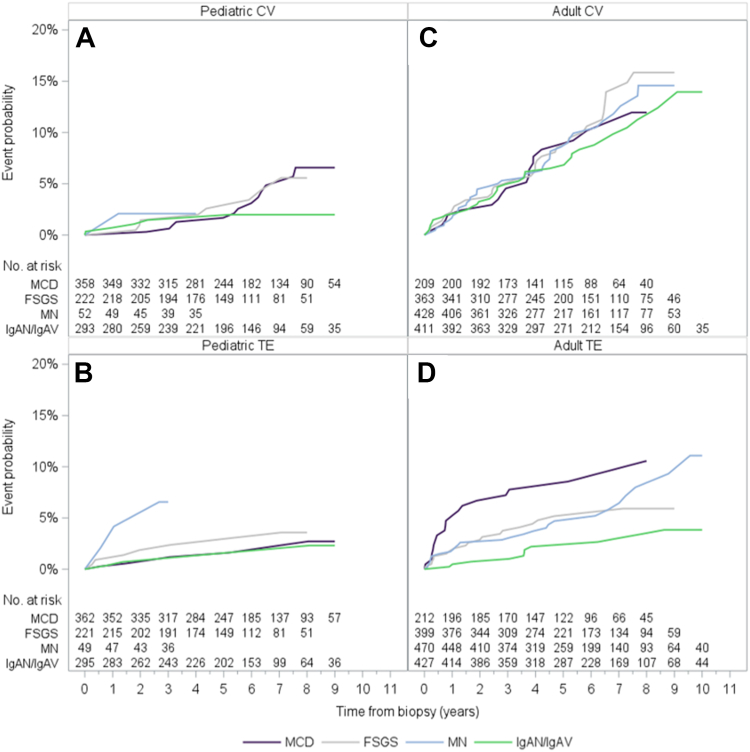
SETTING & PARTICIPANTS: CureGN is a prospective cohort study of children and adults with biopsy-proven minimal change disease (MCD), focal segmental glomerulosclerosis (FSGS), membranous nephropathy (MN), or IgA nephropathy (IgAN)/vasculitis (IgAV). Data from 2,545 children and adults (23% MCD, 23% MN, 25% FSGS, 29% IgAN/IgAV) was analyzed.
Estimated glomerular filtration rate (eGFR), proteinuria, serum albumin, tobacco use, body mass index, hypertension, renin-angiotensin-aldosterone system.
CV and TE events.
Kaplan-Meier curves were used to estimate cumulative incidence, and multivariable Cox proportional hazards models were fitted to estimate associations of histologic diagnosis, age, biological sex, and race. Laboratory and other clinical data were evaluated separately in models adjusted for base model covariates.
Median follow-up time was 4.6 years (IQR 2.7-6.1). The cumulative incidence of first CV and TE event postbiopsy was 3% and 2% in children and 10% and 5% in adults, respectively. No association between GD subtype and risk of CV or TE event was detected. Older age and Black race were associated with higher risk of first CV and TE event {hazard ratio (HR) (95% confidence interval {CI}) per 5 years, CV = 1.17 (1.12-1.23); TE = 1.11 (1.05-1.18); for Black race, CV = 1.62 (1.03-2.56), TE = 2.25 (1.27-4.01)}. Lower eGFR, higher urinary protein-creatinine ratio (UPCR), and lower serum albumin levels at enrollment were associated with higher risk of first CV and TE event (eGFR per 10 mL/min/1.73 m, CV = 0.87 [0.81-0.93], TE = 0.80 [0.73-0.88]; UPCR per mg/mg, CV = 1.04 [1.02-1.07], TE = 1.03 [1.00-1.07]; serum albumin per g/dL, CV = 0.75 [0.59-0.95], TE = 0.71 [0.53-0.96]).
Age of cohort, duration of follow-up.
In the CureGN cohort, elevated risk of incident CV and TE events is associated with severity of kidney disease rather than GD subtype.
心血管(CV)和血栓栓塞(TE)事件是肾小球疾病(GD)已知的并发症,但其发病率和危险因素尚不明确。本分析描述了肾小球肾病治疗(CureGN)网络中的CV和TE结局。
前瞻性队列研究。
CureGN是一项针对经活检证实为微小病变病(MCD)、局灶节段性肾小球硬化(FSGS)、膜性肾病(MN)或IgA肾病(IgAN)/血管炎(IgAV)的儿童和成人的前瞻性队列研究。分析了2545名儿童和成人的数据(23%为MCD,23%为MN,25%为FSGS,29%为IgAN/IgAV)。
估计肾小球滤过率(eGFR)、蛋白尿、血清白蛋白、吸烟、体重指数、高血压、肾素-血管紧张素-醛固酮系统。
CV和TE事件。
采用Kaplan-Meier曲线估计累积发病率,并拟合多变量Cox比例风险模型以估计组织学诊断、年龄、生物学性别和种族的关联。在根据基础模型协变量调整的模型中分别评估实验室和其他临床数据。
中位随访时间为4.6年(四分位间距2.7 - 6.1年)。活检后首次CV和TE事件的累积发病率在儿童中分别为3%和2%,在成人中分别为10%和5%。未检测到GD亚型与CV或TE事件风险之间的关联。年龄较大和黑人种族与首次CV和TE事件的较高风险相关{每5年的风险比(HR)(95%置信区间{CI}),CV = 1.17(1.12 - 1.23);TE = 1.11(1.05 - 1.18);黑人种族,CV = 1.62(1.03 - 2.56),TE = 2.25(1.27 - 4.01)}。入组时较低的eGFR、较高的尿蛋白-肌酐比值(UPCR)和较低的血清白蛋白水平与首次CV和TE事件的较高风险相关(eGFR每降低10 mL/min/1.73 m²,CV = 0.87 [0.81 - 0.93],TE = 0.80 [0.73 - 0.88];UPCR每升高1 mg/mg,CV = 1.04 [1.02 - 1.07],TE = 1.03 [1.00 - 1.07];血清白蛋白每降低1 g/dL,CV = 0.75 [0.59 - 0.95],TE = 0.71 [0.53 - 0.96])。
队列年龄、随访时间。
在CureGN队列中,新发CV和TE事件的风险升高与肾脏疾病的严重程度相关,而非GD亚型。