Wang Zhilin, Shi Zhenghua, Shen Jiayi, Zhang Susu, Fang Yunteng, Hu Wuming, Lv Lingchun
Department of Cardiology, Zhejiang University Lishui Hospital, Hangzhou, China.
Department of Cardiology, Lishui Central Hospital and the Fifth Affiliated Hospital of Wenzhou Medical University, Lishui, China.
Front Cardiovasc Med. 2025 May 30;12:1540750. doi: 10.3389/fcvm.2025.1540750. eCollection 2025.
It is essential to analyze the burden, trends, and inequalities of atrial fibrillation/flutter (AF/AFL) in China and to predict future trends, with the aim of raising awareness about risk factors and exploring strategies to control the significant disease burden.
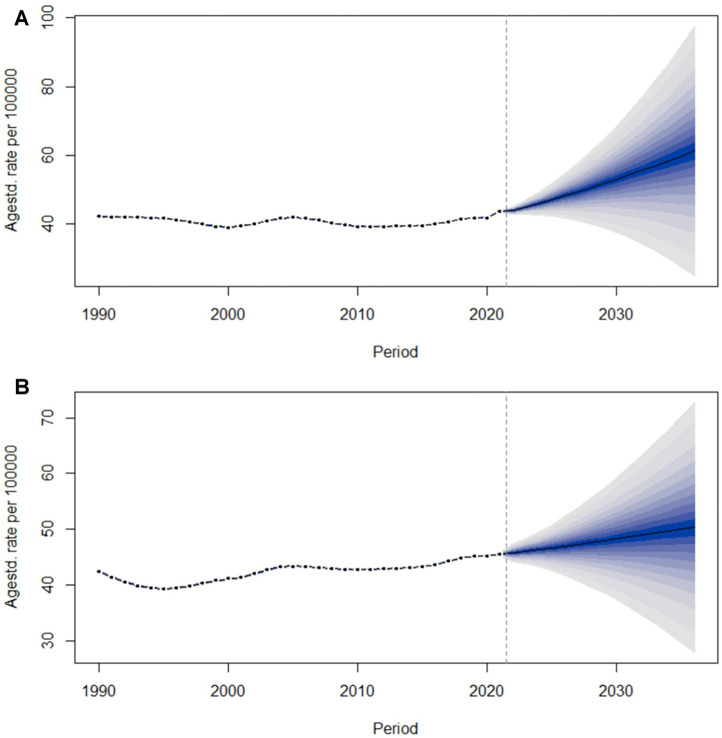
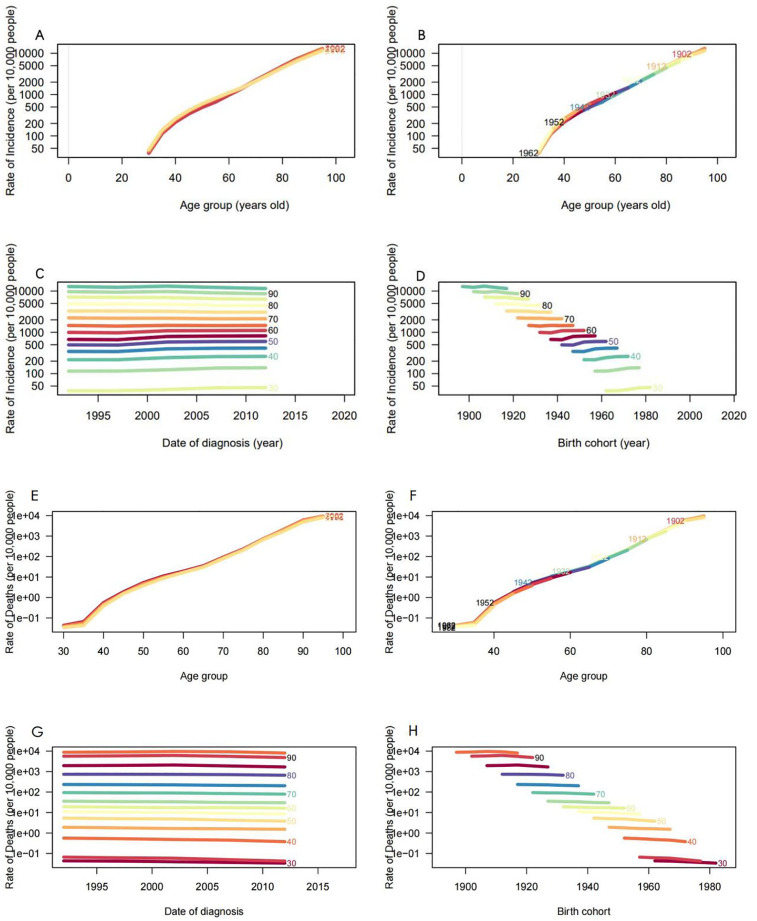
Data pertaining to AF/AFL were extracted from the comprehensive dataset of the Global Burden of Disease, Injuries, and Risk Factors Study 2021 (GBD 2021). Furthermore, we analyzed the epidemiological characteristics of AF/AFL and compared them to global prevalence trends, employing joinpoint regression, decomposition, age-period-cohort (apc), and cross-country inequality analysis methods. Concurrently, we utilized a Bayesian age-period-cohort (BAPC) analysis to forecast the age-standardized incidence rate (ASIR) of AF/AFL in China over the subsequent 15 years.
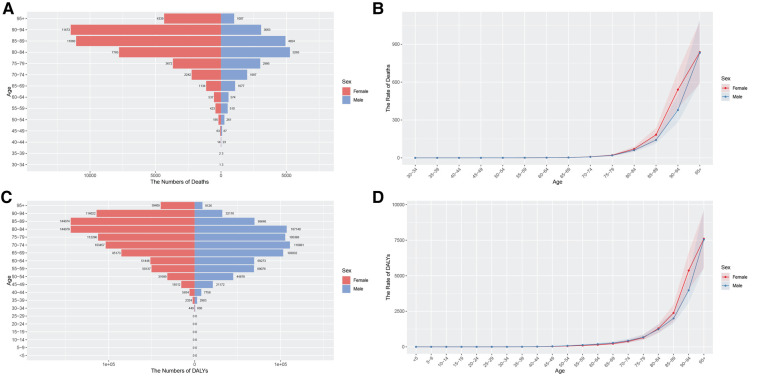
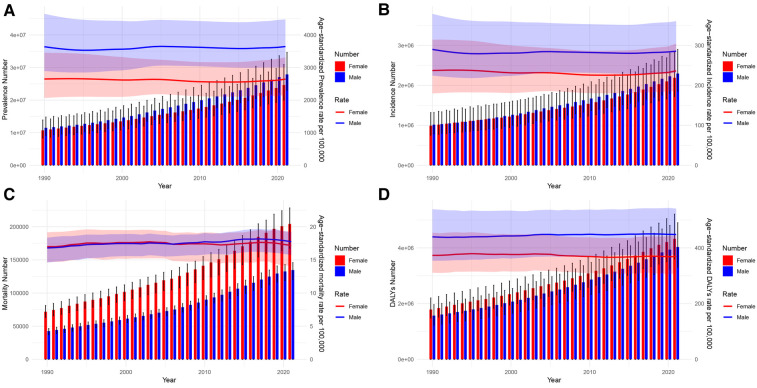
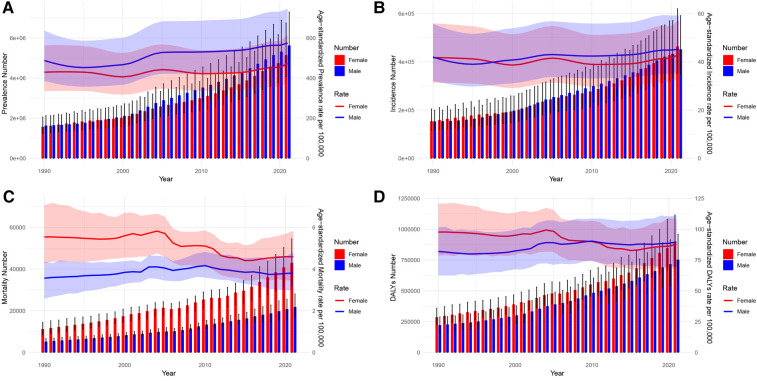
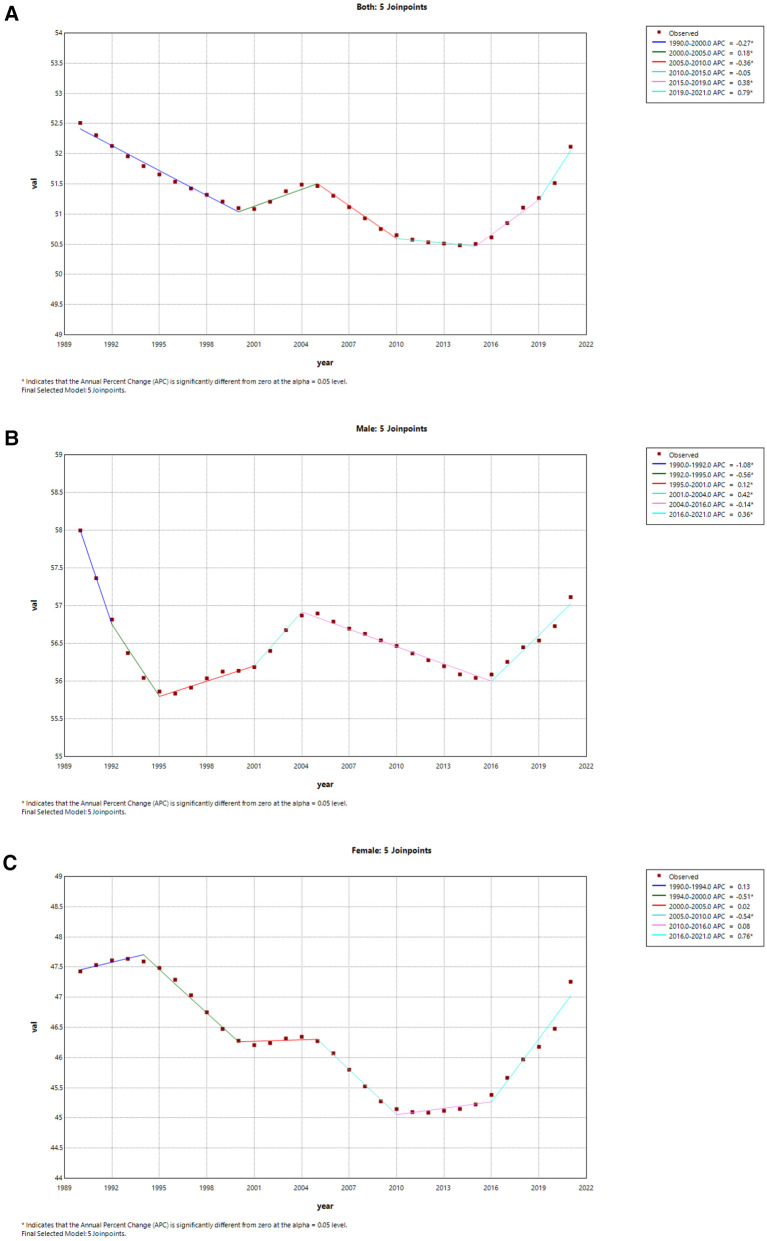
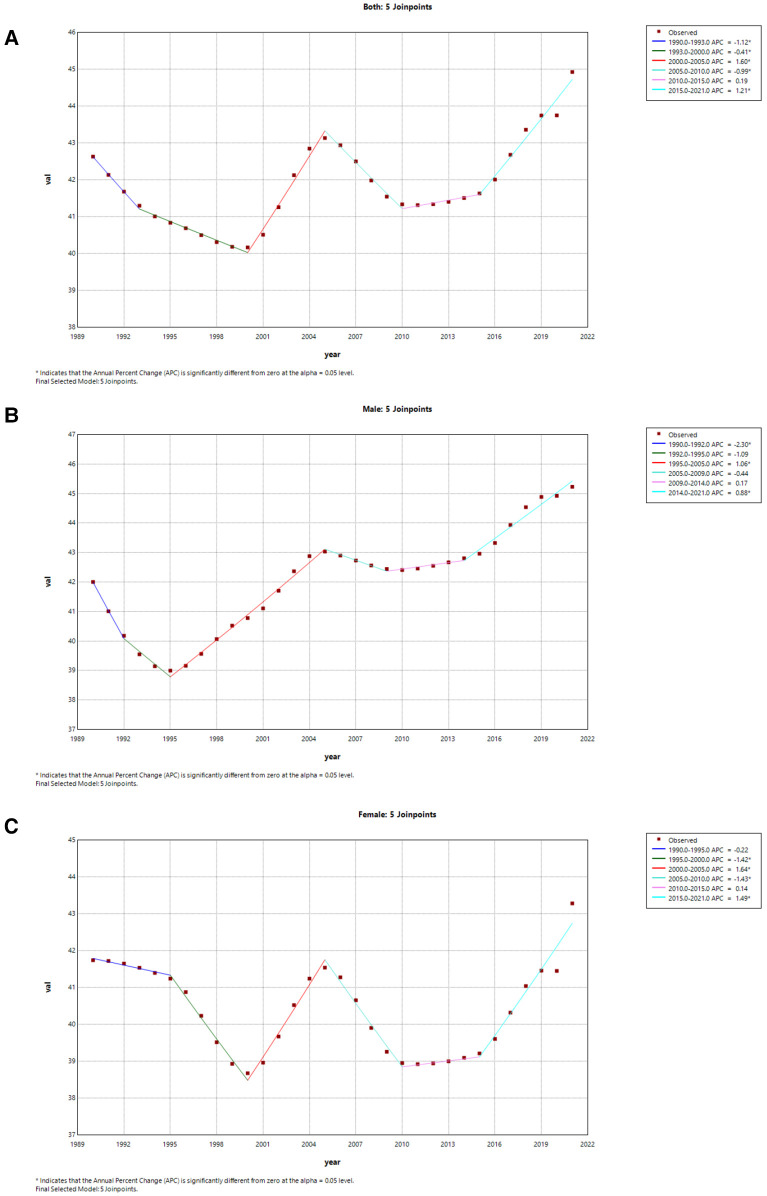
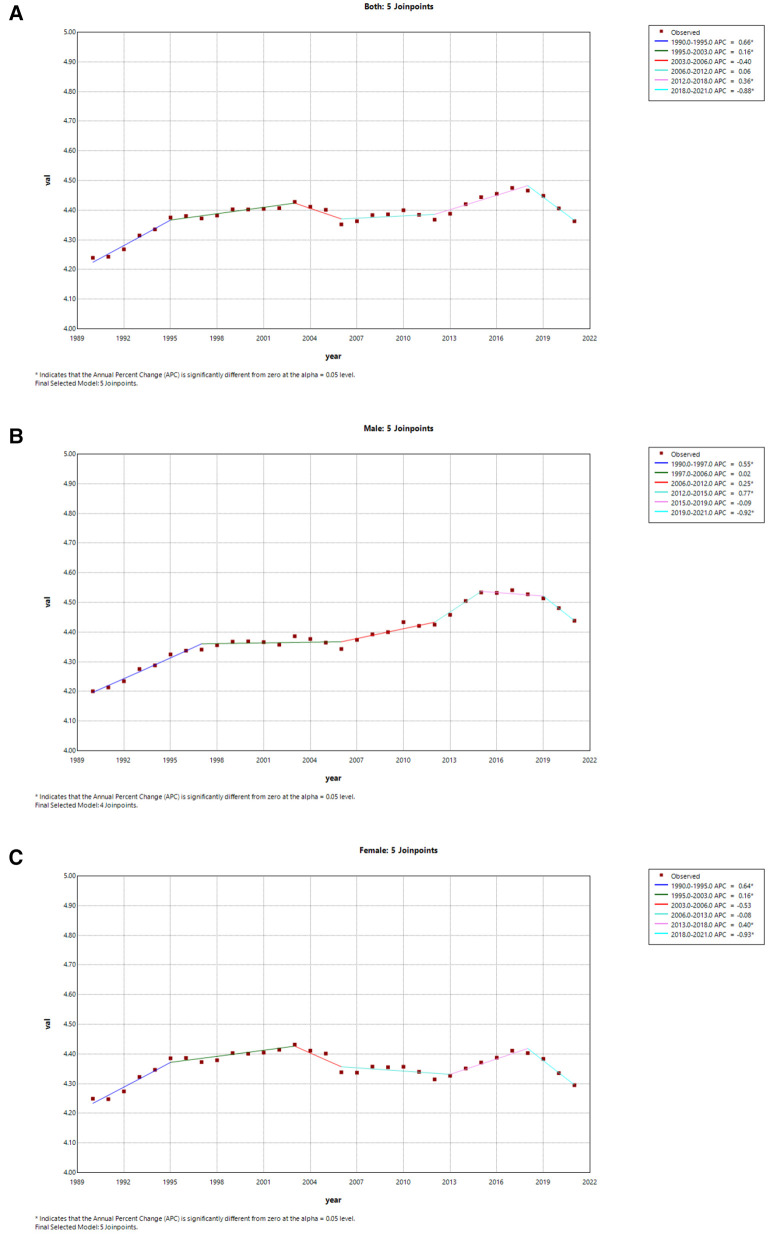
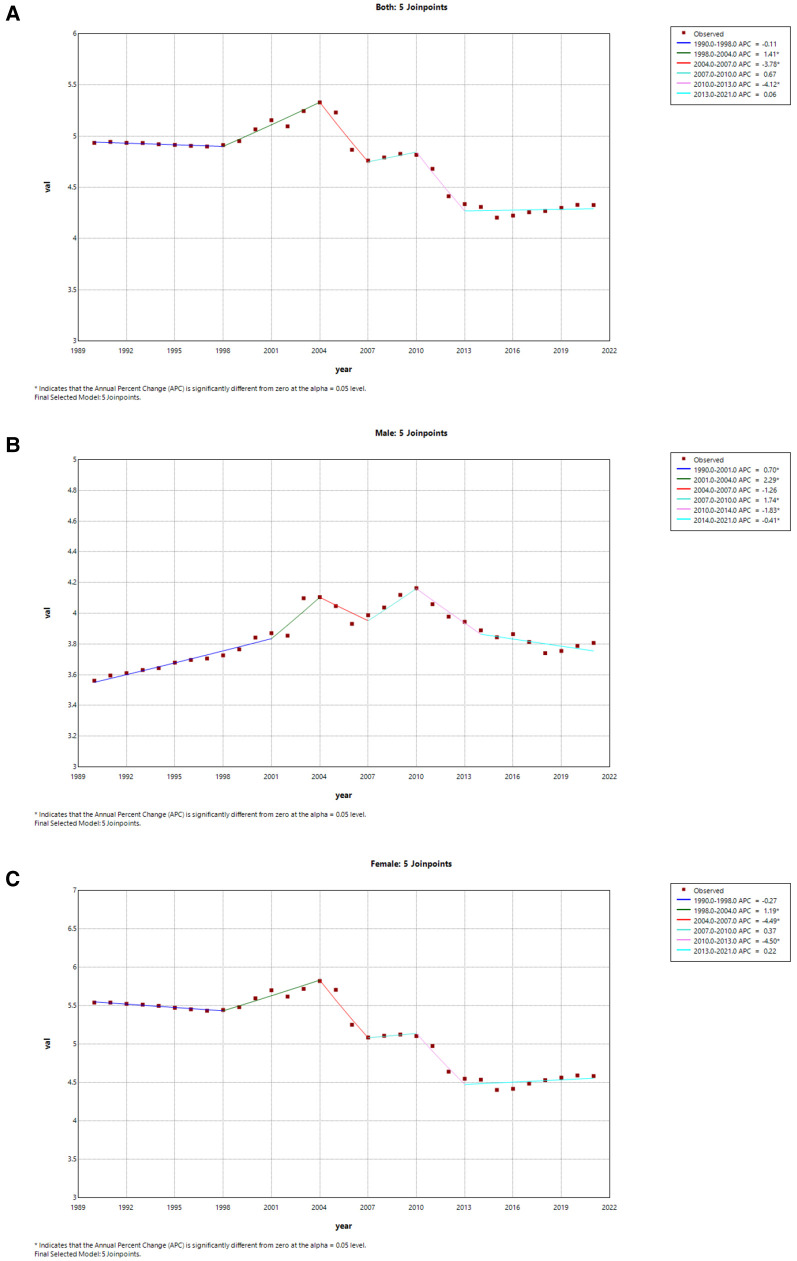
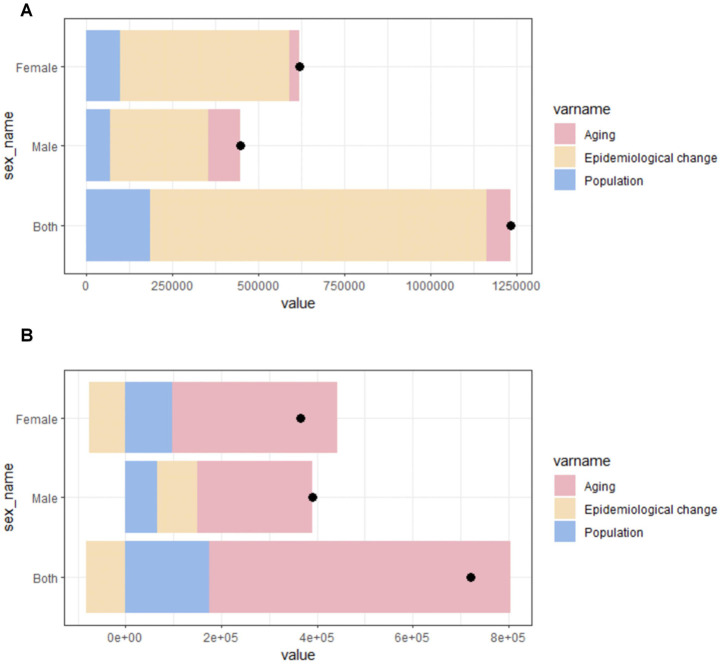
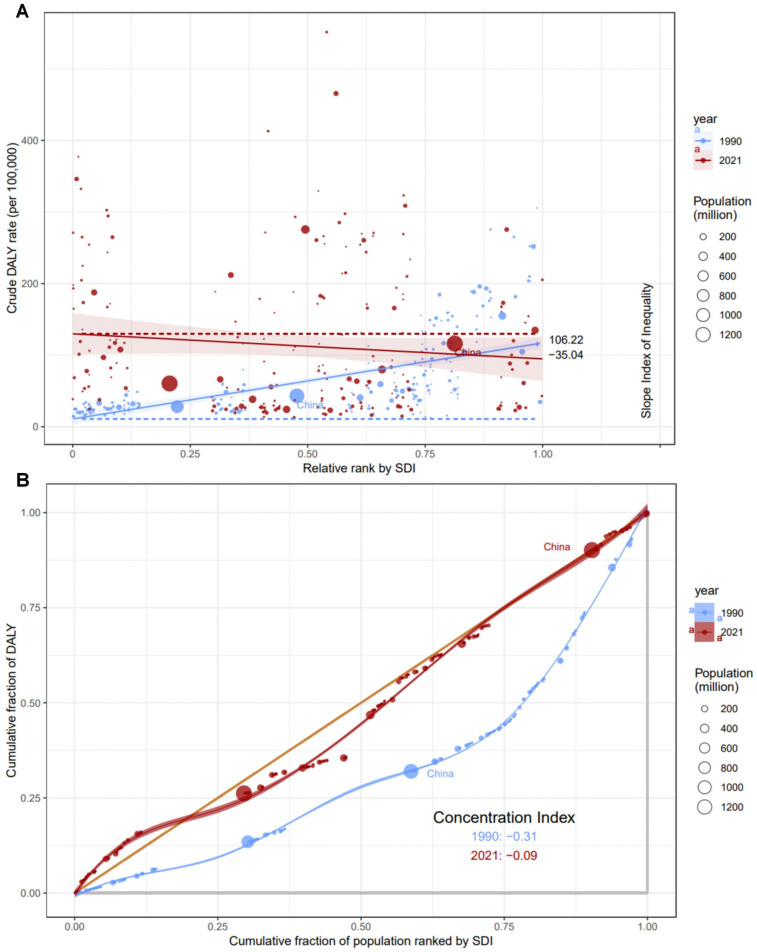
Globally, in 2021, there were 52.55 million [95% uncertainty interval (UI): 43.14 to 64.96] prevalent cases, 4.48 million (95% UI: 3.61 to 5.71) incident cases, 0.34 million (95% UI: 0.28 to 0.37) deaths, and 8.36 million (95% UI: 6.97 to 10.13) DALYs. In China, during the same year, there were 10.78 million (95% UI: 8.53 to 14.01) prevalent cases, 0.92 million (95% UI: 0.71 to 1.20) incident cases, 0.06 million (95% UI: 0.05 to 0.08) deaths, and 1.65 million (95% UI: 1.30 to 2.06) DALYs. The average annual percentage change (AAPC) in age-standardized incidence and mortality rates for AF/AFL were -0.02 (95% CI: -0.05, 0) and 0.11 (95% CI: 0.03, 0.18) globally, and 0.16 (95% CI: 0.05, 0.26) and -0.45 (95% CI: -0.78, -0.12) in China, respectively. Decomposition analysis revealed epidemiological shifts drive incidence rise, aging affects mortality. The Slope Index of Inequality (SII) 2021 was -35.04, and the Concentration Index (CI) was -0.09. The BAPC results indicated that the ASIR for males and females is expected to rise over the next 15 years.
The burden of AF/AFL continues to increase annually. Countries with medium to low Socio-Demographic Index (SDI) have a heavy disease burden. In recent years, the burden in Chinese females has begun to exceed that of males. Without effective measures, the ASIR of AF/AFL is projected to exhibit a continued upward trajectory.
分析中国房颤/房扑(AF/AFL)的负担、趋势和不平等情况,并预测未来趋势至关重要,目的是提高对危险因素的认识并探索控制这一重大疾病负担的策略。
从《2021年全球疾病、伤害和风险因素负担研究》(GBD 2021)的综合数据集中提取与AF/AFL相关的数据。此外,我们分析了AF/AFL的流行病学特征,并使用连接点回归、分解、年龄-时期-队列(apc)和跨国不平等分析方法将其与全球流行趋势进行比较。同时,我们利用贝叶斯年龄-时期-队列(BAPC)分析预测中国未来15年AF/AFL的年龄标准化发病率(ASIR)。
在全球范围内,2021年有5255万例[95%不确定区间(UI):4314万至6496万] 患病率病例、448万例(95% UI:361万至571万)发病率病例、34万例(95% UI:28万至37万)死亡病例和836万例(95% UI:697万至1013万)伤残调整生命年(DALY)。同年在中国,有1078万例(95% UI:853万至1401万)患病率病例、92万例(95% UI:71万至120万)发病率病例、6万例(95% UI:5万至8万)死亡病例和165万例(95% UI:130万至206万)DALY。全球AF/AFL年龄标准化发病率和死亡率的年均变化百分比(AAPC)分别为-0.02(95% CI:-0.05,0)和0.11(95% CI:0.03,0.18),在中国分别为0.16(95% CI:0.05,0.26)和-0.45(95% CI:-0.78,-0.12)。分解分析显示,流行病学转变推动发病率上升,老龄化影响死亡率。2021年不平等斜率指数(SII)为-35.04,集中指数(CI)为-0.09。BAPC结果表明,未来15年男性和女性的ASIR预计将上升。
AF/AFL的负担每年持续增加。社会人口指数(SDI)中低等的国家疾病负担沉重。近年来,中国女性的负担已开始超过男性。若无有效措施,预计AF/AFL的ASIR将持续上升。