Pérez Andrés Cano, Melero Larraitz Orive, Egurbide Jose Félix Larrea, López Jagoba Larrazábal, González Luis Fernández, Mata Roberto Blanco, Meabe Josune Arriola, Mendizábal Leire Artiñano, Goikoetxea Agirre Ane Josune, Blanco Vidal María José, Curiel Javier Ayala, Montes Orbe Pedro María
Cardiology Department, Cruces University Hospital, Baracaldo, Spain.
Infectious Diseases Department, Cruces University Hospital, Baracaldo, Spain.
Int J Cardiol Congenit Heart Dis. 2025 May 13;21:100591. doi: 10.1016/j.ijcchd.2025.100591. eCollection 2025 Sep.
The number of cases of infective endocarditis associated to prosthetic pulmonary valves and pulmonary conduits (PPVIE) is likely to increase in the future. Transthoracic echocardiography (TTE) presents challenges in visualizing lesions suggestive of endocarditis in these patients. However, TTE may provide additional findings, such as prosthetic dysfunction, which can guide the diagnosis of this condition. The main objective of this study is to analyze prosthetic pulmonary valve dysfunction as an echocardiographic manifestation of PPVIE.
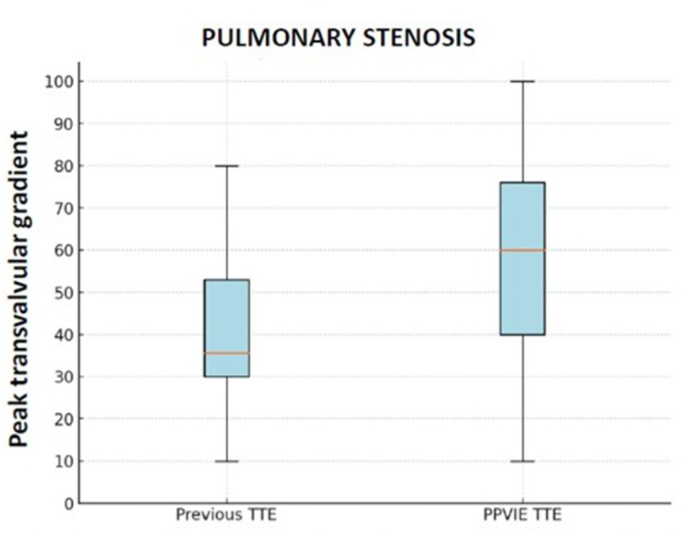
All cases of PPVIE (definite and possible, according to the modified Duke criteria) at Cruces University Hospital (Baracaldo, Spain) between January 2014 and July 2024 were included. Prosthetic dysfunction was defined as a peak transvalvular gradient (PTG) ≥25 mmHg for homografts and ≥40 mmHg for prosthetic pulmonary valves and bovine pulmonary conduits (stenosis) and/or pulmonary regurgitation (PR) moderate or severe. Number of cases of prosthetic dysfunction between the PPVIE episode and prior to the episode were compared. We analyzed the mechanisms of prosthetic dysfunction in the PPVIE episode.
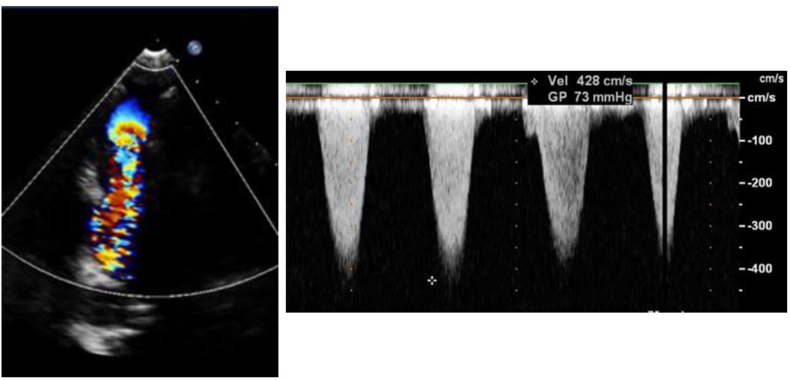
14 cases of PPVIE were identified. In cases prior to the PPVIE episode, 42.9 % had prosthetic dysfunction, while in the PPVIE episode, 92.3 % had prosthetic dysfunction. Stenosis was a more frequent cause of valve dysfunction than PR.
Prosthetic dysfunction (due to stenosis or regurgitation) is a relevant finding in the diagnosis of PPVIE in cases where lesions suggestive of endocarditis are not visualised. Although not included in the Duke criteria, stenosis is a more frequent mechanism of dysfunction than PR.
与人工肺瓣膜和肺导管相关的感染性心内膜炎(PPVIE)病例数未来可能会增加。经胸超声心动图(TTE)在可视化这些患者提示心内膜炎的病变方面存在挑战。然而,TTE可能会提供额外的发现,如人工瓣膜功能障碍,这可以指导对这种疾病的诊断。本研究的主要目的是分析人工肺瓣膜功能障碍作为PPVIE的一种超声心动图表现。
纳入2014年1月至2024年7月在西班牙巴拉卡尔多市克鲁塞斯大学医院确诊的所有PPVIE病例(根据改良的杜克标准确定为确诊和可能病例)。人工瓣膜功能障碍定义为同种异体移植物的跨瓣膜峰值梯度(PTG)≥25mmHg,人工肺瓣膜和牛肺导管的PTG≥40mmHg(狭窄)和/或中度或重度肺反流(PR)。比较PPVIE发作期间和发作前人工瓣膜功能障碍的病例数。我们分析了PPVIE发作期间人工瓣膜功能障碍的机制。
共识别出14例PPVIE病例。在PPVIE发作前,42.9%的病例存在人工瓣膜功能障碍,而在PPVIE发作期间,92.3%的病例存在人工瓣膜功能障碍。狭窄比PR更常导致瓣膜功能障碍。
在未发现提示心内膜炎病变的PPVIE病例诊断中,人工瓣膜功能障碍(由于狭窄或反流)是一个相关发现。虽然狭窄未包括在杜克标准中,但它比PR更常导致功能障碍。