Jansen Gerrit, Irmscher Linda, Jagoda Sunil, Hinkelbein Jochen, May Theodor W, Popp Jakob, Rehberg Sebastian
University Department of Anesthesiology, Intensive Care Medicine, Emergency Medicine and Pain Medicine, Johannes Wesling Klinikum Minden, Ruhr University Bochum, Hans-Nolte-Straße 1, Minden, 32429, Germany.
Department of Anesthesiology and Intensive Care Medicine, Landeskrankenhaus Bludenz, Vlbg. Krankenhaus- Betriebsgesellschaft.m.b.h., Carinagasse 41, Feldkirch, A-6800, Austria.
BMC Anesthesiol. 2025 Jun 19;25(1):296. doi: 10.1186/s12871-025-03168-x.
The aim of this study was to develop a risk calculation model for peri-operative 30-day-mortality in preterm infants in non-cardiac surgery.
Retrospective monocentric follow-up cohort-study of 27,453 pediatric anesthesias at a German university hospital and level one perinatal center between 2008 and 2021 for non-cardiac surgeries. Inclusion criteria were age < 37 post-menstrual weeks at the time of surgery. The primary endpoint was 30-day-mortality after surgery. For statistical analysis, stepwise backwards logistic regressions were performed to identify predictors for 30-day mortality after surgery.
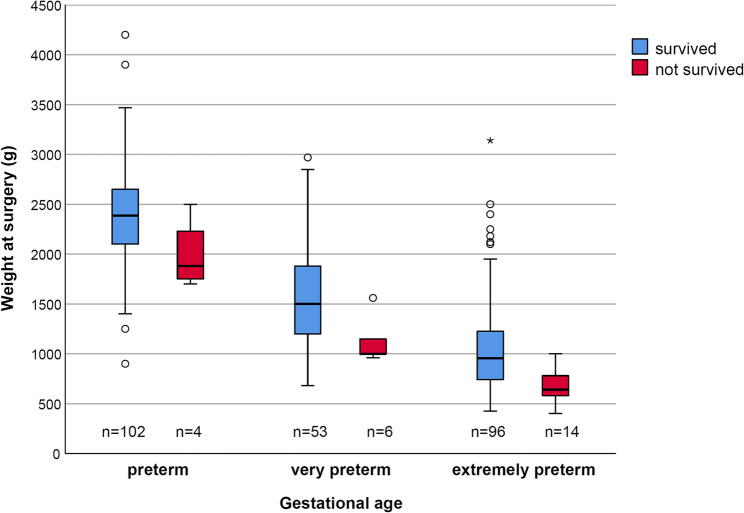
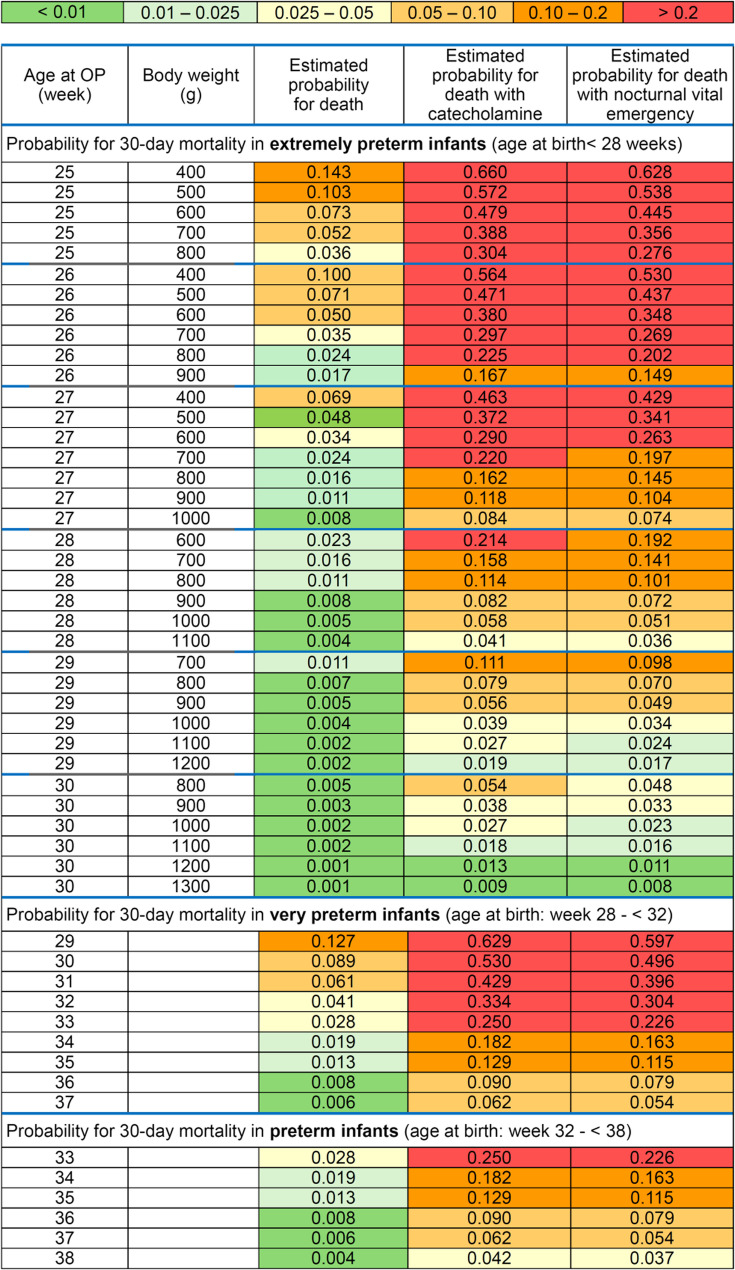
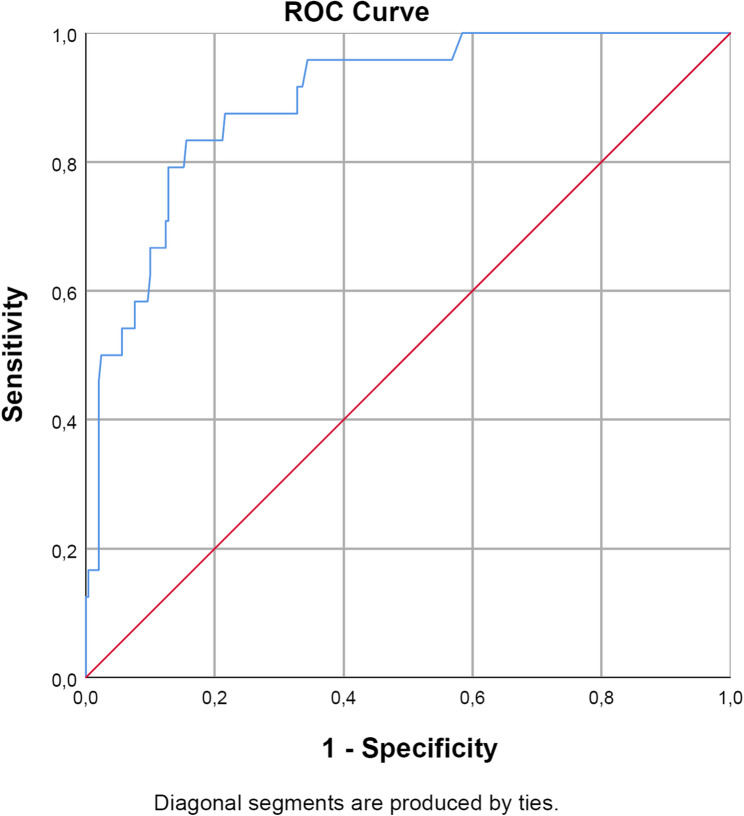
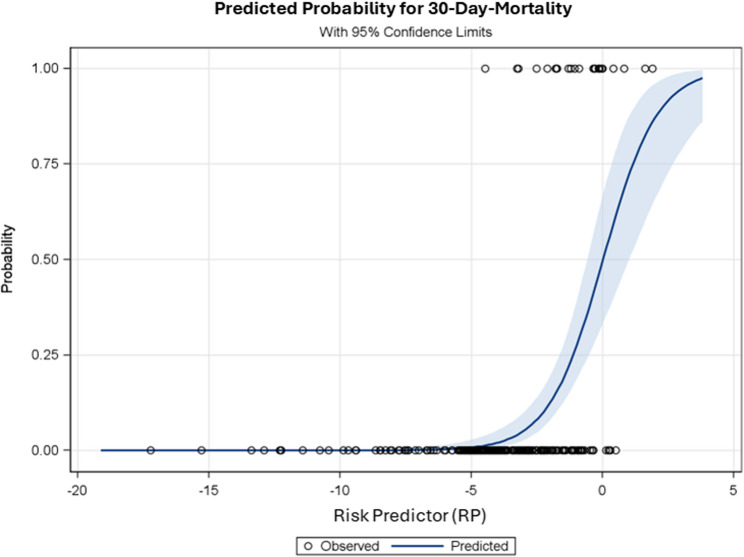
Between 2007 and 2021, 278 preterm infants underwent surgery. The 30-day-mortality was 8.6% (24/278; CI95%:5.6–12.6). A preselection of potential risk factors was based primarily on prior knowledge available from the literature and the results of previously published studies. The final prediction model using a multivariable logistic regression revealed lower post-menstrual age (odds-ratio(OR): 0.67; CI95%: 0.54–0.83) and lower body weight at the time of surgery for extremely preterm infants (OR: 0.024; CI95%: 0.003–0.22), administration of dopamine or norepinephrine or epinephrine (OR: 11.6; CI95%: 3.58–37.7), and life-threatening emergencies between 10pm-7am (OR: 10.1; CI95%: 2.36–43.5) as significant independent risk factors for 30-day-mortality. The Area-Under-The-Receiver-Operating-Characteristic-Curve (0.90; CI95%: 0.85–0.96) showed a good discrimination of the final model. The investigation of the calibration curve ( = 0.99, Spiegelhalter test) and the goodness of fit test ( = 0.85, Hosmer-Lemeshow test) indicated no significant discrepancies between estimated and observed probabilities for the peri-operative 30-day mortality.
Peri-operative 30-day-mortality of preterm infants during non-cardiac surgery is high. The prediction model with easily ascertainable factors as described could be a valuable tool for estimating 30-day-mortality in preterm infants and should be validated in larger populations.
The online version contains supplementary material available at 10.1186/s12871-025-03168-x.
本研究的目的是开发一种用于非心脏手术早产儿围手术期30天死亡率的风险计算模型。
对德国一家大学医院和一级围产期中心2008年至2021年期间27453例非心脏手术的儿科麻醉进行回顾性单中心随访队列研究。纳入标准为手术时月经龄<37周。主要终点是术后30天死亡率。为进行统计分析,采用逐步向后逻辑回归来确定术后30天死亡率的预测因素。
2007年至2021年期间,278例早产儿接受了手术。30天死亡率为8.6%(24/278;95%CI:5.6–12.6)。潜在风险因素的预选主要基于文献中已有的知识和先前发表研究的结果。使用多变量逻辑回归的最终预测模型显示,月经龄较低(优势比[OR]:0.67;95%CI:0.54–0.83)、极早产儿手术时体重较低(OR:0.024;95%CI:0.003–0.22)、使用多巴胺或去甲肾上腺素或肾上腺素(OR:11.6;95%CI:3.58–37.7)以及晚上10点至早上7点之间出现危及生命的紧急情况(OR:10.1;95%CI:2.36–43.5)是30天死亡率的显著独立风险因素。受试者工作特征曲线下面积(0.90;95%CI:0.85–0.96)显示最终模型具有良好的区分度。校准曲线(=0.99,Spiegelhalter检验)和拟合优度检验(=0.85,Hosmer-Lemeshow检验)的调查表明,围手术期30天死亡率的估计概率和观察概率之间无显著差异。
非心脏手术期间早产儿的围手术期30天死亡率很高。所述的具有易于确定因素的预测模型可能是估计早产儿30天死亡率的有价值工具,应在更大人群中进行验证。
在线版本包含可在10.1186/s12871-025-03168-x获取的补充材料。