Lopes César Vivian, Pereira-Lima Júlia Fernanda Semmelmann, Salerno Marianna Lins de Souza, Luzzatto Felipe
Department of Gastroenterology and Digestive Endoscopy, Santa Casa Hospital, Porto Alegre, Brazil.
Department of Endocrinology, Santa Casa Hospital, Porto Alegre, Brazil.
Ochsner J. 2025 Summer;25(2):123-132. doi: 10.31486/toj.24.0115.
Papillary thyroid carcinoma, the most common differentiated thyroid cancer, has an indolent clinical course and a good prognosis. Metastases to the gastrointestinal tract account for <1% of all distant metastases, and the pancreas is an extremely rare site for metastasis from thyroid cancer.
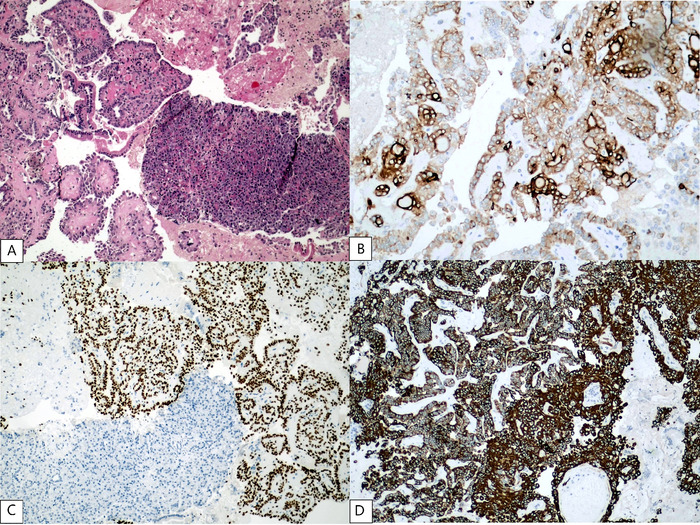
We report the case of a patient who developed a pancreatic metastasis from a classic variant papillary thyroid carcinoma 11 years after total thyroidectomy, cervical lymphadenectomy, and radioactive iodine ablation. The patient experienced increased thyroglobulin levels, and abdominal computed tomography scan revealed a lesion in the uncinate process of the pancreas. Tissue samples obtained by endoscopic ultrasound-guided biopsy were positive for thyroglobulin and thyroid transcription factor 1. Because the patient was not a candidate for surgery, the metastatic lesion was not iodine-avid, and tyrosine kinase inhibitors could not be offered because of tumor-related symptoms, the patient was treated with stereotactic body radiotherapy only. The patient died almost 2 years after the diagnosis of metastatic papillary thyroid carcinoma to the pancreas (13 years after total thyroidectomy for the primary cancer).
If pancreatic lesions are discovered during regular follow-up of patients who have previously been treated for papillary thyroid carcinoma, pancreatic metastasis must be considered, and imaging procedures other than whole-body iodine scintigraphy are required. Histopathology and iodine avidity will define the best therapeutic strategy. Radioactive iodine ablation should be considered for iodine-avid metastases, and surgery or tyrosine kinase inhibitors are promising options for non-iodine-avid lesions.
乳头状甲状腺癌是最常见的分化型甲状腺癌,临床病程进展缓慢,预后良好。胃肠道转移占所有远处转移的比例不到1%,胰腺是甲状腺癌转移极为罕见的部位。
我们报告一例患者,在全甲状腺切除、颈部淋巴结清扫及放射性碘消融术后11年,出现了源自经典型乳头状甲状腺癌的胰腺转移。患者甲状腺球蛋白水平升高,腹部计算机断层扫描显示胰腺钩突部有一病灶。经内镜超声引导下活检获取的组织样本甲状腺球蛋白和甲状腺转录因子1呈阳性。由于该患者不适合手术,转移病灶不摄取碘,且因肿瘤相关症状无法使用酪氨酸激酶抑制剂,故仅对患者进行了立体定向体部放疗。该患者在被诊断为胰腺转移性乳头状甲状腺癌后近2年死亡(距原发癌全甲状腺切除术后13年)。
如果在既往接受过乳头状甲状腺癌治疗的患者定期随访期间发现胰腺病变,必须考虑胰腺转移,且需要全身碘闪烁扫描以外的影像学检查。组织病理学和碘摄取情况将确定最佳治疗策略。对于摄取碘的转移灶应考虑放射性碘消融,而手术或酪氨酸激酶抑制剂是治疗不摄取碘病灶的有前景的选择。