Jannelli Gianpaolo, Polinelli Francesco, Giardina Antonella, Cuzzolin Marco, Calvanese Francesco, Cabrilo Ivan, Paun Luca, Tessitore Enrico
Division of Neurosurgery, Department of Clinical Neurosciences, Geneva University Hospitals, University of Geneva Faculty of Medicine, Geneva, Switzerland.
Department of Neurosurgery, Neurocenter of Southern Switzerland, Ente Ospedaliero Cantonale, Lugano, Switzerland.
Brain Spine. 2025 May 30;5:104285. doi: 10.1016/j.bas.2025.104285. eCollection 2025.
Recurrent lumbar disc herniation (RLDH) is defined as the reappearance, following initial discectomy, of disc material and pain after a period of at least six symptom-free months. Redo surgery is usually considered following unsuccessful conservative management or in the presence of neurological deficits.
Given the lack of consensus on the ideal surgical strategy for RLDH, we conducted this study to evaluate when lumbar fusion (LF) should be considered in the treatment of RLDH.
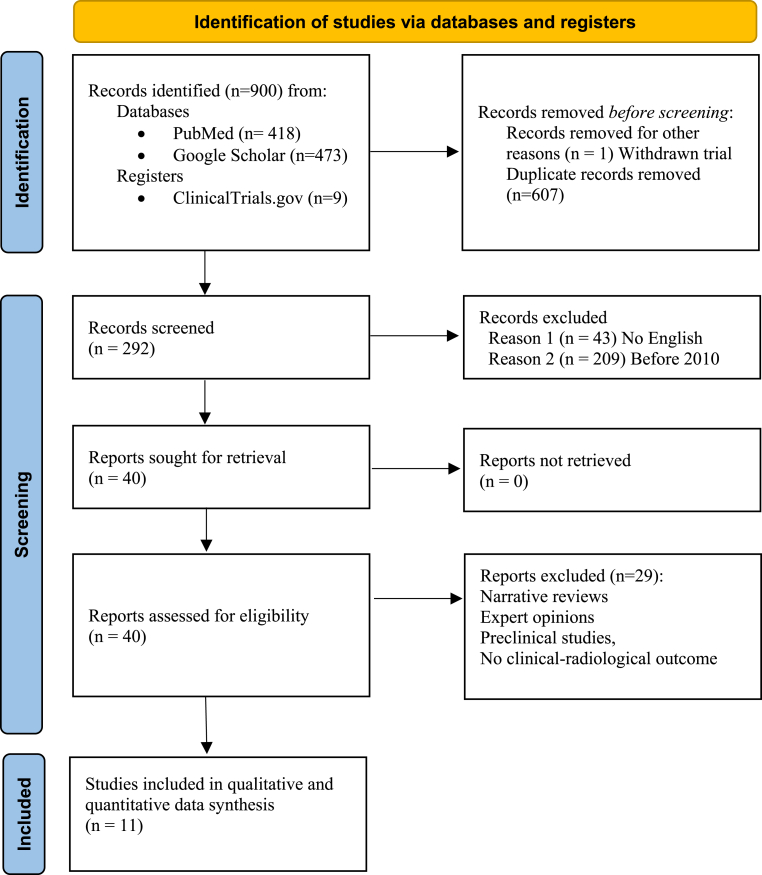
A literature search was conducted on PubMed, Google Scholar and clinicaltrials.gov focusing on the treatment of recurrent disc herniation using microdiscectomy alone or through fusion. The quality of the studies was evaluated using the Newcastle-Ottawa Quality Assessment Scale and Cochrane Risk of Bias Tool 2.0. The weighted mean difference was calculated for both binary and continuous outcomes.
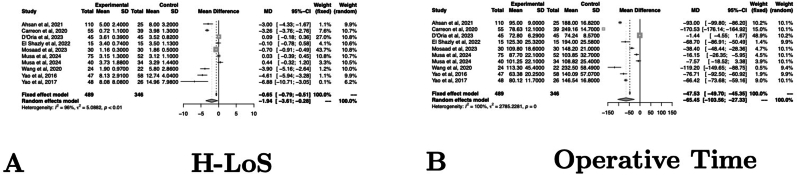
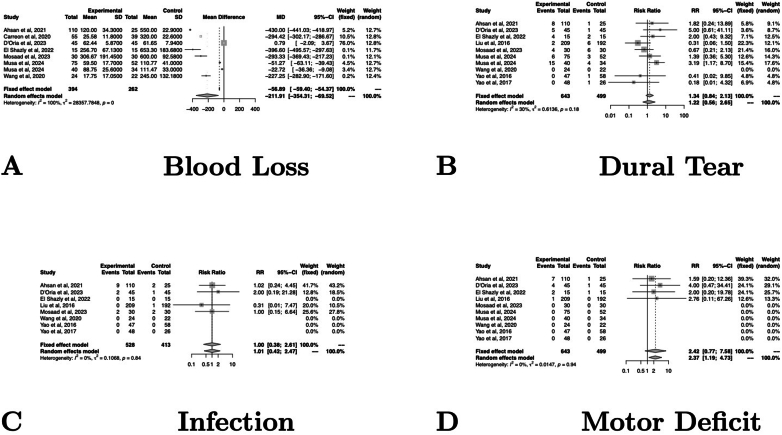
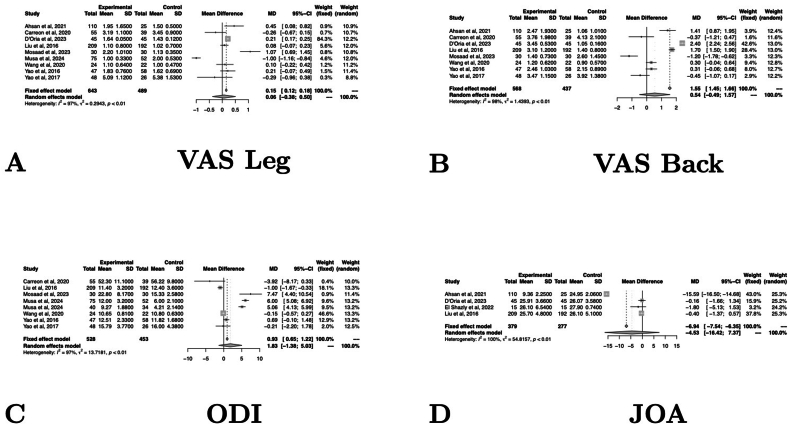
This resulted in a list of 900 references, from which 11 studies were identified as meeting the inclusion criteria for the study. There were four prospective studies and seven retrospective studies. A comparison of LF and redo discectomy (RD) revealed no significant differences in clinical outcome scores. LF resulted in significantly higher intraoperative blood loss, longer hospitalizations and longer surgeries. No further differences were identified.
Both LF and RD represent safe and effective treatment options in first RLDH. The choice of surgical strategy should integrate the eventual co-existence of clinical and radiological features of segmental instability, as well subjective aspects, such as surgeons' training and patient preference.
复发性腰椎间盘突出症(RLDH)的定义为,在初次椎间盘切除术后,经过至少6个月无症状期后,椎间盘物质再次出现并伴有疼痛。通常在保守治疗失败或存在神经功能缺损时考虑再次手术。
鉴于对于RLDH理想手术策略缺乏共识,我们开展了本研究以评估在RLDH治疗中何时应考虑腰椎融合术(LF)。
在PubMed、谷歌学术和clinicaltrials.gov上进行文献检索,重点关注单独使用显微椎间盘切除术或通过融合术治疗复发性椎间盘突出症。使用纽卡斯尔-渥太华质量评估量表和Cochrane偏倚风险工具2.0评估研究质量。计算二元和连续结局的加权平均差。
这产生了一份900篇参考文献的列表,从中确定了11项研究符合该研究的纳入标准。有4项前瞻性研究和7项回顾性研究。LF与再次椎间盘切除术(RD)的比较显示临床结局评分无显著差异。LF导致术中失血量显著增加、住院时间延长和手术时间延长。未发现进一步差异。
LF和RD都是首次RLDH安全有效的治疗选择。手术策略的选择应综合考虑节段性不稳定的临床和放射学特征的最终共存情况,以及诸如外科医生培训和患者偏好等主观因素。