Fang Hongzhi, Ji Huihua, Shi Changjian, Zhou Benrui, Xu Jie, Luo Yuli, Li Yunfei
Department of Urology, Renmin Hospital, Hubei University of Medicine, Shiyan, Hubei, China.
Front Oncol. 2025 Jun 6;15:1592406. doi: 10.3389/fonc.2025.1592406. eCollection 2025.
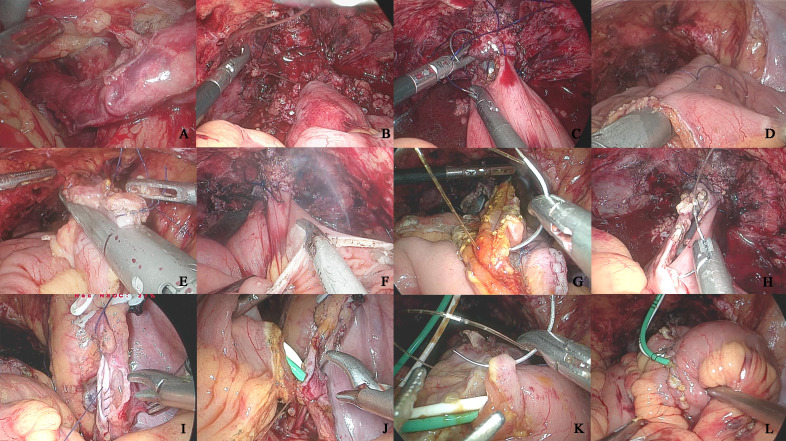
To explore the feasibility of combined laparoscopic radical cystectomy (LRC) and intracorporeal urinary diversion (ICUD) in the treatment of bladder cancer, as well as the influencing factors related to complications.
A retrospective study was conducted on 116 bladder cancer patients who underwent LRC at our facility between January 2019 and December 2023. Based on the different urinary diversion methods, 78 patients received extracorporeal urinary diversion (ECUD), while 38 patients underwent intracorporeal urinary diversion (ICUD). The two groups were compared in terms of clinicopathologic data, perioperative outcomes, postoperative tumor control, complication rates, and their influencing factors.
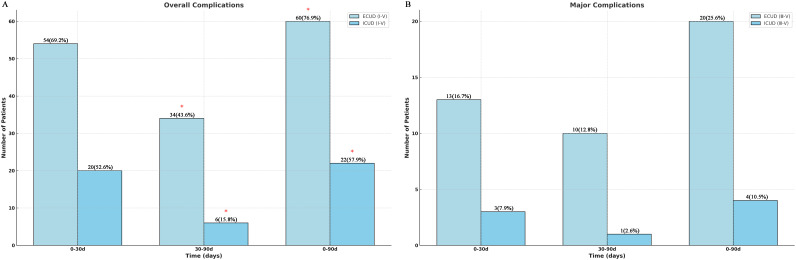
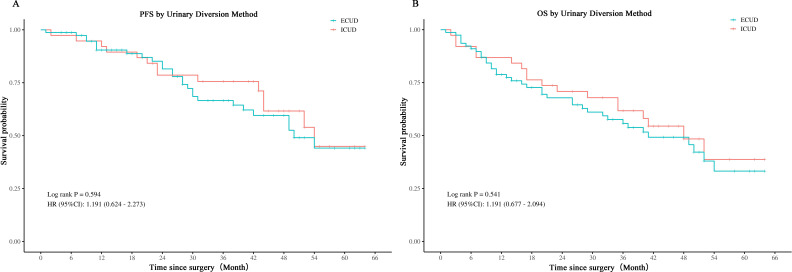
No statistically significant differences were observed between the two groups in terms of median total operative time, hospital stay, perioperative transfusion rate, and short-term oncological outcomes. Compared to the ECUD group, the ICUD group experienced less intraoperative blood loss (200 ml vs. 350 ml) and an earlier start to postoperative liquid diet intake (4 days vs. 5 days) (p < 0.05). A total of 24 cases of ≥III grade complications occurred within 90 days postoperatively, with 20 cases in the ECUD group and 4 in the ICUD group. There was no significant difference in the incidence of ≥III grade complications between the two groups (p > 0.05). Sepsis was the most common major complication. Logistic regression analysis identified smoking history, diabetes, and intraoperative blood loss as independent risk factors for ≥III complications.
ICUD is a secure and effective method with advantages such as improved postoperative bowel recovery, reduced intraoperative blood loss, and fewer overall postoperative complications. Furthermore, major complications are influenced by multiple risk factors and should be carefully considered during preoperative and postoperative management.
探讨腹腔镜根治性膀胱切除术(LRC)联合体内尿流改道术(ICUD)治疗膀胱癌的可行性以及与并发症相关的影响因素。
对2019年1月至2023年12月在我院接受LRC的116例膀胱癌患者进行回顾性研究。根据不同的尿流改道方法,78例患者接受体外尿流改道术(ECUD),38例患者接受体内尿流改道术(ICUD)。比较两组患者的临床病理资料、围手术期结局、术后肿瘤控制情况、并发症发生率及其影响因素。
两组患者在中位总手术时间、住院时间、围手术期输血率和短期肿瘤学结局方面无统计学显著差异。与ECUD组相比,ICUD组术中出血量更少(200 ml对350 ml),术后开始流质饮食的时间更早(4天对5天)(p<0.05)。术后90天内共发生24例≥Ⅲ级并发症,ECUD组20例,ICUD组4例。两组≥Ⅲ级并发症的发生率无显著差异(p>0.05)。脓毒症是最常见的主要并发症。Logistic回归分析确定吸烟史、糖尿病和术中出血量是≥Ⅲ级并发症的独立危险因素。
ICUD是一种安全有效的方法,具有术后肠道恢复改善、术中出血量减少和术后总体并发症较少等优点。此外,主要并发症受多种危险因素影响,术前和术后管理时应仔细考虑。