Lee Hyung Gon, Bom Joon-Suk, Lee Leyeoin, Kim Joungmin
Department of Anesthesiology and Pain Medicine, Chonnam National University Medical School, Chonnam National University Hospital, 160 Baekseo-Ro, Dong-Gu, Gwangju, 61469, Korea.
Department of Anesthesiology and Pain Medicine, Hwasun Chonnam National University Hospital, Hwasun, Korea.
J Cardiothorac Surg. 2025 Jun 25;20(1):273. doi: 10.1186/s13019-025-03491-x.
Thyroid storm (TS) is an endocrine emergency requiring aggressive medical management. In severe cases, hemodynamic instability may necessitate extracorporeal membrane oxygenation (ECMO) support as a bridge to definitive surgical treatment. ECMO is categorized into two types: venoarterial (V-A) ECMO, which provides both cardiac and pulmonary support, and venovenous (V-V) ECMO, which supports only pulmonary function. Surgery is generally not recommended for patients with unstable TS due to the high risk of complications, even when ECMO support is in place. Here, we present a case of a 44-year-old man initially improved with V-A ECMO for TS with cardiogenic shock, but later developed refractory hypoxemia due to pulmonary thromboembolism (PTE). He subsequently underwent emergency thyroidectomy with continuous support from V-V ECMO.
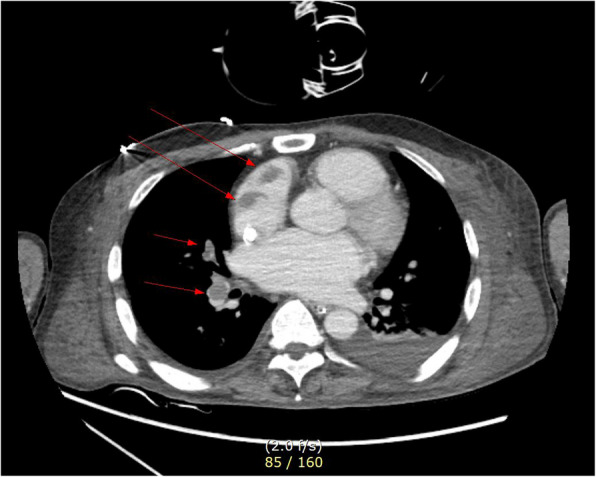
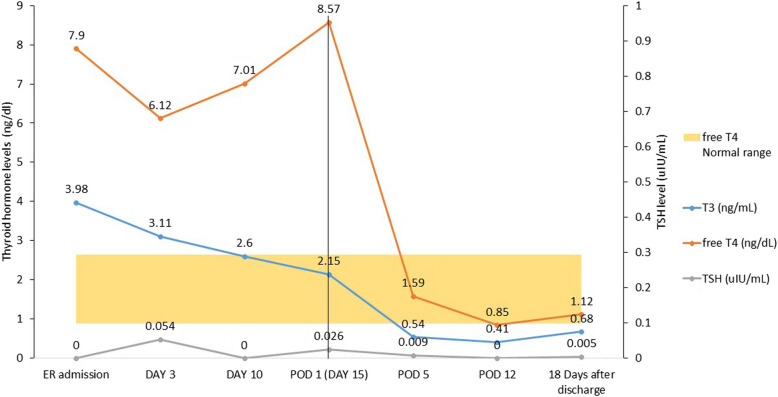
A 44-year-old man presented to our hospital with complaints of palpitations. He had a recent history of coronavirus disease of 2019 (COVID-19) infection, which may have exacerbated undiagnosed hyperthyroidism, leading to thyroid storm and cardiogenic shock (left ventricular ejection fraction [LVEF], 13%). Heart failure improved with immediate medical management and V-A ECMO for 4 days, resulting in LVEF, 30%. V-A ECMO provide both respiratory and cardiac support, allowing myocardial recovery. Although the patient's cardiac output improved, uncontrolled tachycardia persisted. Medical treatment for hyperthyroidism-associated tachycardia was continued after V-A ECMO weaning but failed to achieve adequate rate control. Ten days after weaning V-A ECMO, the patient suddenly developed pulmonary thromboembolism and hypoxia despite ongoing heparinization. To manage refractory hypoxia, V-V ECMO was initiated, as it exclusively provides respiratory support. Given that persistent TS was the underlying cause of the patient's instability, we proceeded with thyroidectomy under general anesthesia with V-V ECMO support, despite the associated risks. On postoperative day 4, the patient was successfully weaned off V-V ECMO. By postoperative day 18, he was discharged without complications, with an improved LVEF of 52.5%.
This is the first reported case of total thyroidectomy performed while on V-V ECMO support for TS complicated by PTE. Although V-V ECMO is more susceptible to hemodynamic instability than V-A ECMO, this case demonstrates that thyroidectomy can be successfully performed with appropriate anesthesia management. Additionally, careful selection of the ECMO modality based on the patient's condition is crucial for optimal management.
甲状腺风暴(TS)是一种内分泌急症,需要积极的药物治疗。在严重情况下,血流动力学不稳定可能需要体外膜肺氧合(ECMO)支持作为确定性手术治疗的桥梁。ECMO分为两种类型:静脉-动脉(V-A)ECMO,提供心脏和肺部支持;静脉-静脉(V-V)ECMO,仅支持肺功能。由于并发症风险高,即使有ECMO支持,一般也不建议对TS不稳定的患者进行手术。在此,我们报告一例44岁男性患者,最初因心源性休克的TS接受V-A ECMO治疗后病情改善,但后来因肺血栓栓塞症(PTE)出现难治性低氧血症。随后,他在V-V ECMO的持续支持下接受了急诊甲状腺切除术。
一名44岁男性因心悸主诉前来我院就诊。他近期有2019冠状病毒病(COVID-19)感染史,这可能使未被诊断的甲状腺功能亢进症加重,导致甲状腺风暴和心源性休克(左心室射血分数[LVEF],13%)。通过立即的药物治疗和V-A ECMO治疗4天,心力衰竭得到改善,LVEF为30%。V-A ECMO提供呼吸和心脏支持,使心肌得以恢复。尽管患者的心输出量有所改善,但无法控制的心动过速持续存在。V-A ECMO撤机后继续进行甲亢相关心动过速的药物治疗,但未能实现充分的心率控制。V-A ECMO撤机10天后,尽管持续使用肝素,患者突然发生肺血栓栓塞和低氧血症。为了处理难治性低氧血症,启动了V-V ECMO,因为它专门提供呼吸支持。鉴于持续性TS是患者不稳定的根本原因,尽管存在相关风险,我们在V-V ECMO支持下进行全身麻醉下的甲状腺切除术。术后第4天,患者成功撤掉V-V ECMO。到术后第18天,他无并发症出院,LVEF提高到52.5%。
这是第一例报告的在V-V ECMO支持下对合并PTE的TS进行全甲状腺切除术的病例。尽管V-V ECMO比V-A ECMO更容易出现血流动力学不稳定,但该病例表明,通过适当的麻醉管理可以成功进行甲状腺切除术。此外,根据患者情况仔细选择ECMO模式对于优化管理至关重要。