Bockholt Sebastian, Schneider Kristian Nikolaus, Gosheger Georg, Smolle Maria Anna, Deventer Niklas, Andreou Dimosthenis, Theil Christoph
Department of Orthopedics and Tumor Orthopedics, Muenster University Hospital, Albert-Schweitzer-Campus 1, 48149 Muenster, Germany.
Department of Orthopaedics and Traumatology, Medical University of Graz, Auenbruggerplatz 5, 8036 Graz, Austria.
Cancers (Basel). 2025 Jun 13;17(12):1982. doi: 10.3390/cancers17121982.
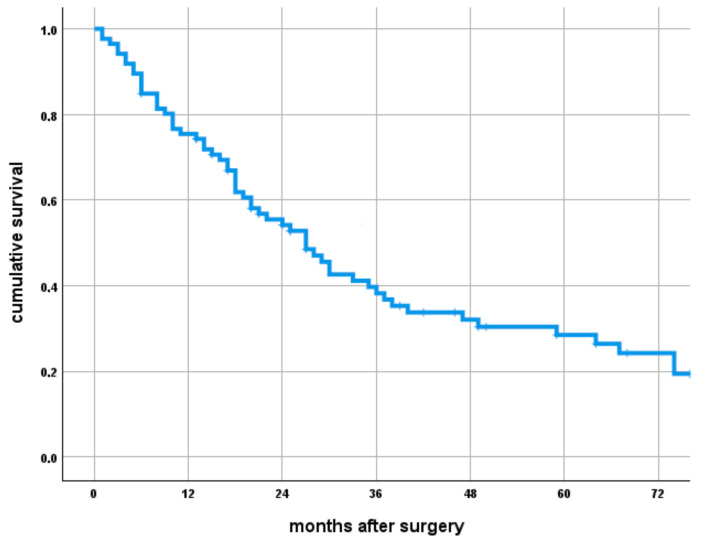
Long bone metastases are common in patients with metastatic renal cell carcinoma (RCC). One potential surgical treatment option is resection and megaprosthetic reconstruction. However, implant complications and survival are poorly understood. This study analyzes patient and implant survival as well as associated risk factors. This is a retrospective study from a single academic center, analyzing 86 patients that underwent resection and megaprosthetic reconstruction performed between 1993 and 2017. The most common location of megaprosthetic reconstruction was the proximal femur (PFR) in 38% (33 of 86) of patients. We calculated overall patient survival and associated risk factors using the Kaplan-Meier method and implant survivorship using a competing risk analysis. A total of 73% (63/86) of patients died of their disease after a median of 19 (IQR 9-37) months following surgery, and a median of 71 (IQR 31-132) months after the initial diagnosis of RCC. The overall survival probability was 29% (95% CI 18-40%) five years after surgery. The five-year risk of revision surgery (within a competing risk framework) was 18% (95% CI 11-28). A total of 8% (7 of 86) of patients underwent an exchange of the implant itself. Patients with total bone replacements had a higher revision risk (SHR 19.46 (95% CI 6.9-54.9), < 0.01). Furthermore, the revision risk was higher with increasing reconstruction length per mm (SHR 1.01 (95% CI 1.01-1.02), = 0.03) and prolonged surgical time per minute (SHR: 1.01 (95% CI 1.0-1.02), < 0.01). Local postoperative radiation treatment (RTX) was associated with an increased risk for revisions (SHR 2.59 (95% CI 0.96-6.95), = 0.06). Modular megaprostheses demonstrated a fairly low risk of implant revision although postoperative radiation therapy and total bone replacements are associated with an increased risk.
长骨转移在转移性肾细胞癌(RCC)患者中很常见。一种潜在的手术治疗选择是切除并进行大假体重建。然而,植入物并发症和生存率尚不清楚。本研究分析了患者和植入物的生存率以及相关危险因素。这是一项来自单一学术中心的回顾性研究,分析了1993年至2017年间接受切除和大假体重建的86例患者。大假体重建最常见的部位是股骨近端(PFR),占38%(86例中的33例)。我们使用Kaplan-Meier方法计算患者总生存率和相关危险因素,并使用竞争风险分析计算植入物生存率。共有73%(63/86)的患者在术后中位19个月(IQR 9-37)、RCC初始诊断后中位71个月(IQR 31-132)死于疾病。术后五年总生存概率为29%(95%CI 18-40%)。五年内翻修手术风险(在竞争风险框架内)为18%(95%CI 11-28)。共有8%(86例中的7例)患者进行了植入物本身的更换。全骨置换患者的翻修风险更高(标准化风险比19.46(95%CI 6.9-54.9),<0.01)。此外,每毫米重建长度增加,翻修风险更高(标准化风险比1.01(95%CI 1.01-1.02),P = 0.03)以及手术时间每分钟延长,翻修风险更高(标准化风险比:1.01(95%CI 1.0-1.02),<0.01)。局部术后放射治疗(RTX)与翻修风险增加相关(标准化风险比2.59(95%CI 0.96-6.95),P = 0.06)。模块化大假体显示出植入物翻修风险相当低,尽管术后放射治疗和全骨置换与风险增加相关。