Boppana Leela Krishna Teja, Isern Samantha, Romero Kaitlyn N, Ferreira Jason, Garvan Gerard, Ashby Tracy
Division of Pulmonary and Critical Care Medicine, University of Florida-Jacksonville, 655 W 8th Street, Jacksonville, FL 32209, USA.
Division of Internal Medicine, University of Florida-Jacksonville, Jacksonville, FL 32209, USA.
J Clin Med. 2025 Jun 10;14(12):4086. doi: 10.3390/jcm14124086.
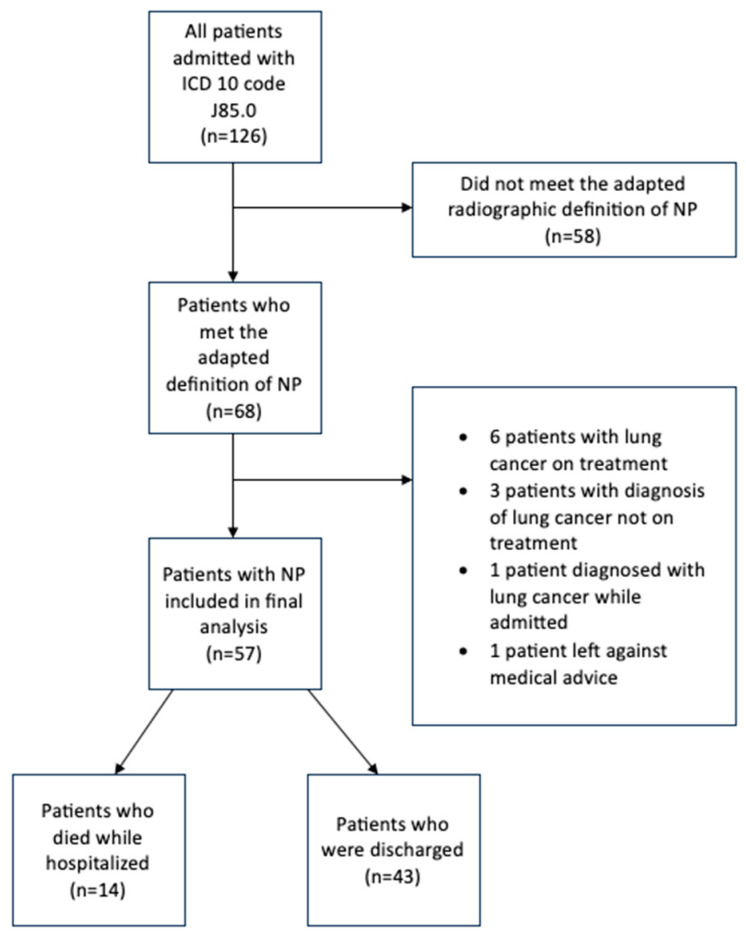
: Necrotizing pneumonia (NP) is an uncommon, severe complication of community-acquired pneumonia (CAP) associated with increased hospital length of stay and high morbidity and mortality. Although this entity was described several decades ago, there is no consensus on radiological criteria for diagnosis, optimal antibiotic duration, or data on clinical outcomes in adults. Given the paucity of data on this entity, a retrospective cohort study was conducted at our institution to evaluate factors associated with all-cause mortality, hospital length of stay, and duration of antibiotics. : An IRB-approved retrospective cohort analysis was conducted through electronic health record review at a tertiary academic center at the University of Florida-Jacksonville. The electronic health record was queried for a list of all hospitalizations from 1 January 2016 to 31 December 2023 with an International Classification of Diseases, 10th revision diagnosis code of J85.0 (gangrene and necrosis of the lung). The primary outcome was all-cause mortality, and secondary outcomes were hospital length of stay and duration of antibiotics. : A total of 57 patients met the definition of necrotizing pneumonia and were included in our study. Fourteen (24.6%) patients died while hospitalized. The mean length of hospital stay was 26.6 days, and the median duration of antibiotics was 28 days. The only statistically significant predictor in the model of all-cause mortality was the requirement of mechanical ventilation, with mortality being 27 times more likely in patients requiring mechanical ventilation (OR 27.6 (95% CI (2.6924, 671.9648)); = 0.011). : To our knowledge, this is the largest cohort of adult patients with NP in the literature. We found that mortality was 24.6%, with the requirement of mechanical ventilation associated with 27 times higher risk of mortality on multivariable logistic regression analysis.
坏死性肺炎(NP)是社区获得性肺炎(CAP)一种罕见的严重并发症,与住院时间延长及高发病率和死亡率相关。尽管该疾病在几十年前就已被描述,但对于其诊断的影像学标准、最佳抗生素使用疗程或成人临床结局数据尚无共识。鉴于关于该疾病的数据匮乏,我们机构开展了一项回顾性队列研究,以评估与全因死亡率、住院时间和抗生素使用疗程相关的因素。
通过对佛罗里达大学杰克逊维尔分校一所三级学术中心的电子健康记录进行审查,开展了一项经机构审查委员会批准的回顾性队列分析。在电子健康记录中查询了2016年1月1日至2023年12月31日期间所有住院患者的列表,其国际疾病分类第十次修订版诊断代码为J85.0(肺坏疽和坏死)。主要结局是全因死亡率,次要结局是住院时间和抗生素使用疗程。
共有57例患者符合坏死性肺炎的定义并纳入我们的研究。14例(24.6%)患者在住院期间死亡。平均住院时间为26.6天,抗生素使用疗程的中位数为28天。全因死亡率模型中唯一具有统计学意义的预测因素是机械通气需求,需要机械通气的患者死亡率高27倍(比值比27.6(95%置信区间(2.6924,671.9648));P = 0.011)。
据我们所知,这是文献中最大的成年坏死性肺炎患者队列。我们发现死亡率为24.6%,在多变量逻辑回归分析中,机械通气需求与死亡率高27倍相关。