Ramachandran Sujith, Maharjan Shishir, Lin Liang-Yuan, Bentley John P, McGwin Gerald, Eriator Ike, Bhattacharya Kaustuv, Yang Yi
Department of Pharmacy Administration, School of Pharmacy, University of Mississippi, University, Mississippi, USA.
Center for Pharmaceutical Marketing & Management, School of Pharmacy, University of Mississippi, University, Mississippi, USA.
Innov Aging. 2025 Mar 11;9(6):igaf028. doi: 10.1093/geroni/igaf028. eCollection 2025.
Long-term opioid therapy (LTOT) is frequently used for management of chronic noncancer pain, but its associations with increased risks of overdose and mortality have necessitated an evaluation of strategies for tapering or discontinuation. The process of opioid tapering is complex due to associated withdrawal symptoms and potential adverse outcomes. Thus, understanding tapering patterns and associated factors is vital for optimizing pain management, especially for vulnerable older adults.
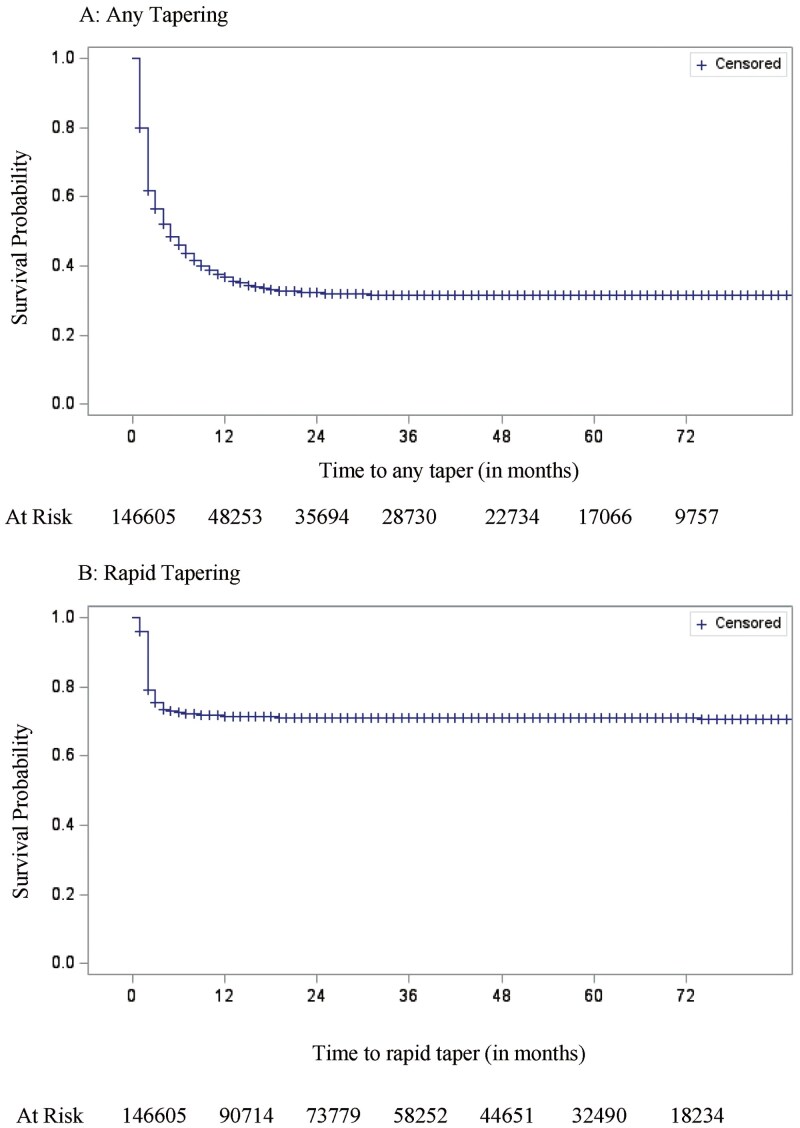
This cohort study used the 5% national sample of Medicare administrative claims data from 2012 to 2019. The study cohort consisted of individuals aged 65 and older on LTOT. The key outcomes were time until any tapering or rapid tapering of opioids. Various predictor variables, including sociodemographic and clinical factors, were examined. Survival curves were plotted, and Cox proportional hazards models were used for data analysis.
The study cohort included 146,605 Medicare beneficiaries on LTOT, of which the largest percentages were aged 65-74 years (48.5%), women (68.0%), and non-Hispanic White (82.3%). Within the first year of LTOT use, nearly 1 in 2 individuals experienced any tapering, and about 1 in 4 individuals experienced rapid tapering. Presence of multiple chronic noncancer pain conditions, hepatic impairment, sleep disorders, higher baseline opioid dose, and LTOT initiation after 2016 were associated with increased rate of both any tapering and rapid tapering. The release of the 2016 CDC guideline was associated with a 45% and 64% increase in the hazards of any tapering and rapid tapering, respectively.
This study estimated the incidence rate and predictors of opioid tapering among older adults in the United States. Combined with rates of opioid prescribing and prevalence of chronic pain, these epidemiological data are crucial for identifying and improving the safety and effectiveness of pain management among older adults.
长期阿片类药物治疗(LTOT)常用于慢性非癌性疼痛的管理,但它与过量用药和死亡风险增加相关,因此有必要评估减药或停药策略。由于存在相关的戒断症状和潜在不良后果,阿片类药物减药过程较为复杂。因此,了解减药模式及相关因素对于优化疼痛管理至关重要,尤其是对于脆弱的老年人。
这项队列研究使用了2012年至2019年医疗保险行政索赔数据的5%全国样本。研究队列包括接受LTOT治疗的65岁及以上个体。主要结局是直至阿片类药物出现任何减药或快速减药的时间。研究了各种预测变量,包括社会人口统计学和临床因素。绘制了生存曲线,并使用Cox比例风险模型进行数据分析。
研究队列包括146,605名接受LTOT治疗的医疗保险受益人,其中最大比例为65 - 74岁(48.5%)、女性(68.0%)和非西班牙裔白人(82.3%)。在LTOT使用的第一年内,近二分之一的个体经历了任何减药,约四分之一的个体经历了快速减药。存在多种慢性非癌性疼痛病症、肝功能损害、睡眠障碍、较高的基线阿片类药物剂量以及2016年后开始LTOT治疗与任何减药和快速减药的发生率增加相关。2016年美国疾病控制与预防中心(CDC)指南的发布分别使任何减药和快速减药的风险增加了45%和64%。
本研究估计了美国老年人中阿片类药物减药的发生率及预测因素。结合阿片类药物处方率和慢性疼痛患病率,这些流行病学数据对于识别和提高老年人疼痛管理的安全性和有效性至关重要。