Holt Margrethe Flesvig, Michelsen Annika E, Flø August, Khan Yusuf, Bjørnø Vilde Karoline, Skjelland Mona, Bjerkeli Vigdis, Paus Benedicte, Kvitting John-Peder, Halvorsen Bente, Wien Tale Norbye, Raki Melinda, Gullestad Lars, Aukrust Pål, Broch Kaspar, Ueland Thor, Gude Einar
Department of Cardiology, Oslo University Hospital, Rikshospitalet, Oslo, Norway; Research Institute of Internal Medicine, Oslo University Hospital, Rikshospitalet, Oslo, Norway; Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway.
Research Institute of Internal Medicine, Oslo University Hospital, Rikshospitalet, Oslo, Norway; Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway.
JACC Adv. 2025 May 30;4(6 Pt 1):101828. doi: 10.1016/j.jacadv.2025.101828.
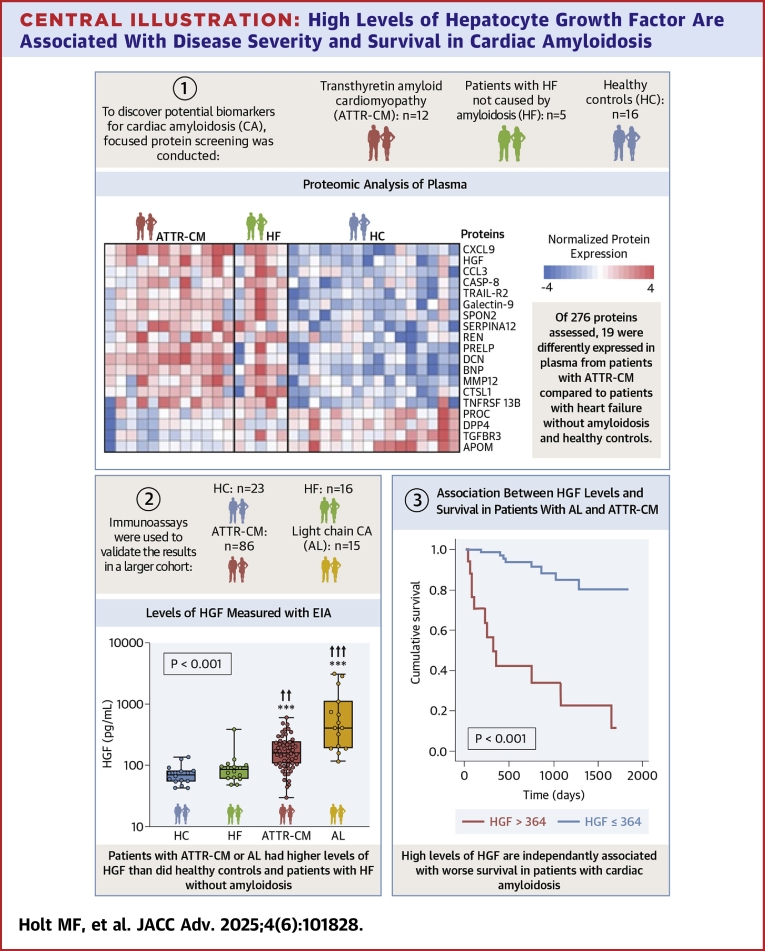
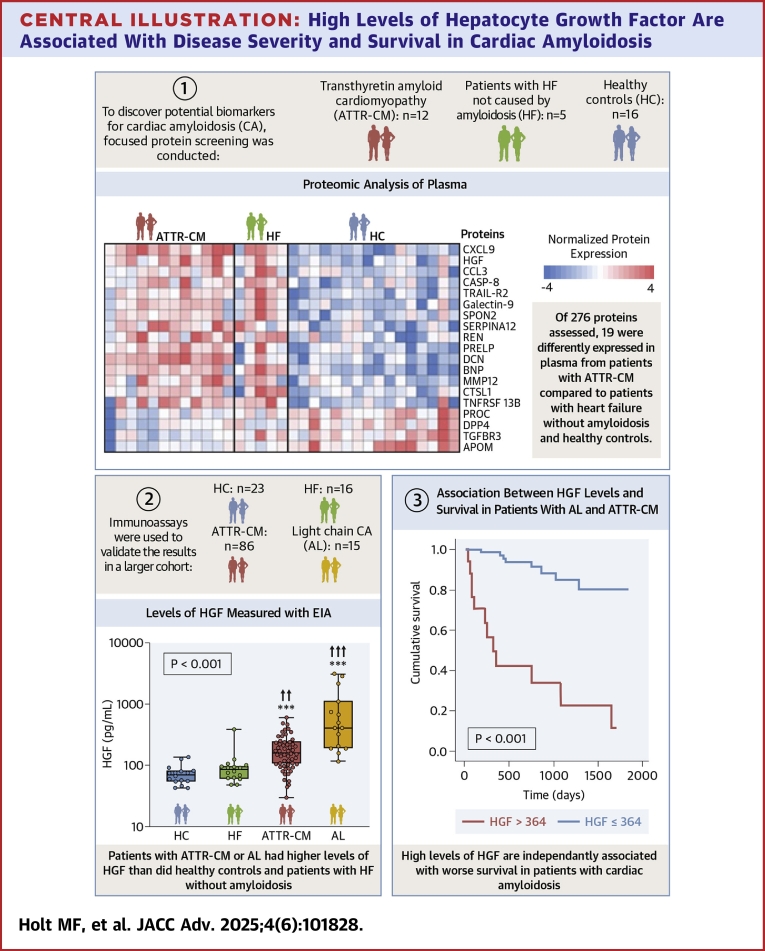
It is important to reduce diagnostic delays for patients with cardiac amyloidosis (CA). Plasma biomarkers could streamline the diagnostic process and enhance prognostic accuracy.
The authors aimed to identify circulating biomarkers capable of differentiating patients with CA from patients with heart failure (HF) and no amyloidosis. Additionally, we assessed whether these markers were associated with patient outcomes.
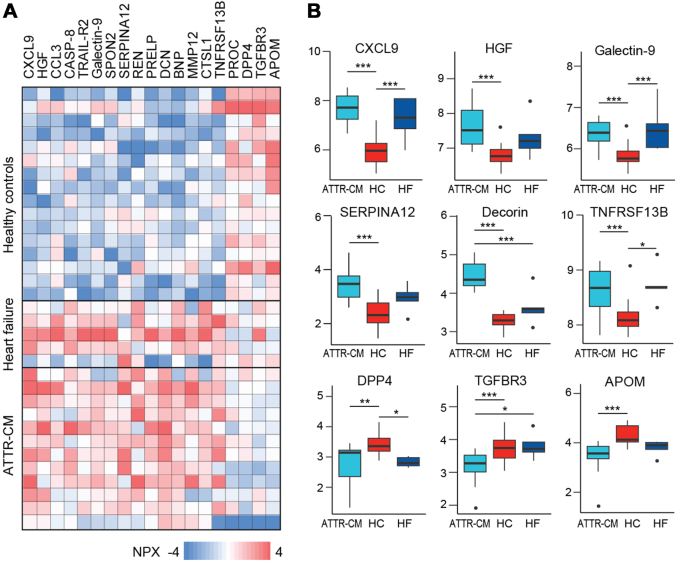
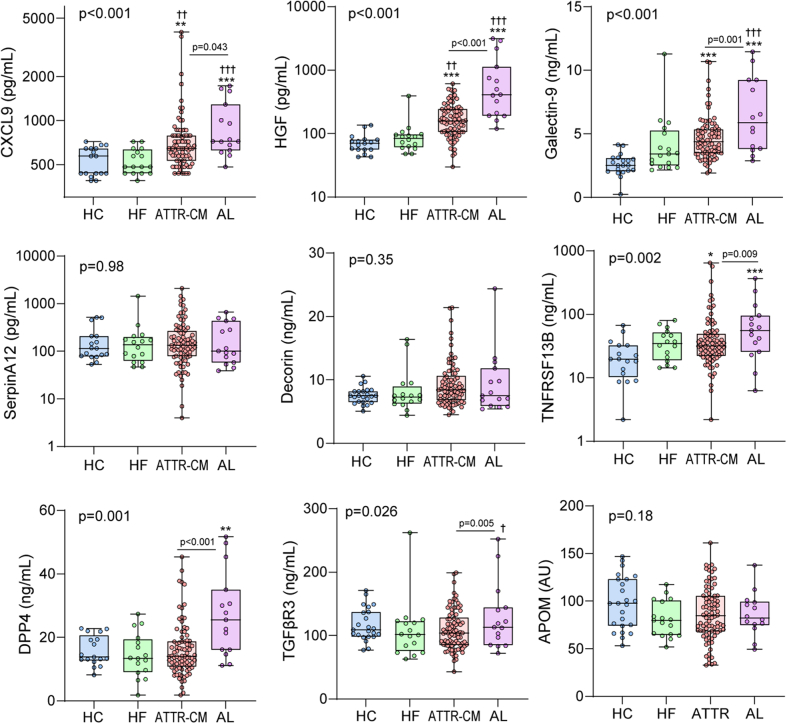
We performed focused protein screening in 12 patients with transthyretin CA, 5 patients with HF, and 16 healthy controls (HCs). To validate the findings, we used immunoassays to measure levels of differentially regulated proteins in a larger sample of 86 patients with transthyretin CA, 15 patients with light-chain CA, 16 patients with HF, and HCs. We compared protein levels between groups using multivariable general linear models. Associations between protein levels and all-cause mortality were assessed by receiver operating characteristic analysis.
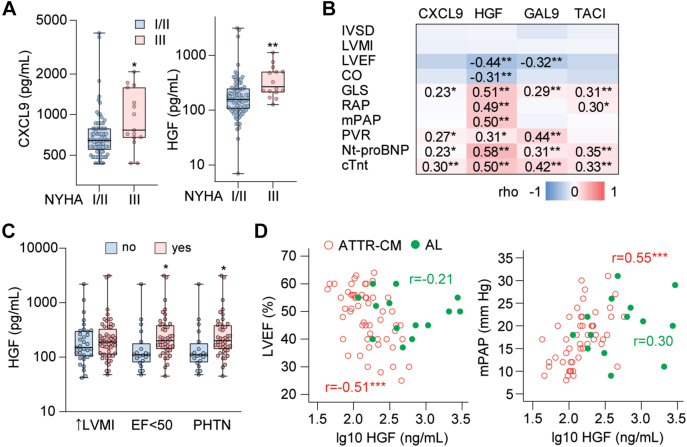
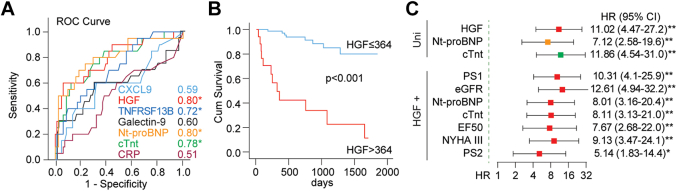
We identified 99 candidate proteins by proteomic screening. In the validation sample, 4 of these markers were higher in CA than in HCs. Levels of C-X-C motif chemokine ligand 9 and hepatocyte growth factor (HGF) were also higher in CA than in HF. HGF correlated with measures of cardiac function in patients with transthyretin and light chain CA. HGF had a good discriminatory ability for predicting all-cause mortality (area under the curve = 0.80, P < 0.001), similar to those of N-terminal pro-B-type natriuretic peptide and troponin T.
Plasma HGF is a promising screening tool for CA. Higher levels of HGF are associated with more severe HF and worse prognosis in patients with CA.
减少心脏淀粉样变性(CA)患者的诊断延迟很重要。血浆生物标志物可简化诊断过程并提高预后准确性。
作者旨在识别能够区分CA患者与心力衰竭(HF)且无淀粉样变性患者的循环生物标志物。此外,我们评估了这些标志物是否与患者预后相关。
我们对12例转甲状腺素蛋白CA患者、5例HF患者和16例健康对照(HC)进行了重点蛋白质筛查。为了验证研究结果,我们使用免疫测定法测量了86例转甲状腺素蛋白CA患者、15例轻链CA患者、16例HF患者和HC的更大样本中差异调节蛋白的水平。我们使用多变量一般线性模型比较了各组之间的蛋白质水平。通过受试者工作特征分析评估蛋白质水平与全因死亡率之间的关联。
通过蛋白质组学筛查,我们鉴定出99种候选蛋白。在验证样本中,这些标志物中有4种在CA中高于HC。CA中C-X-C基序趋化因子配体9和肝细胞生长因子(HGF)的水平也高于HF。HGF与转甲状腺素蛋白和轻链CA患者的心脏功能指标相关。HGF对预测全因死亡率具有良好的鉴别能力(曲线下面积 = 0.80,P < 0.001),与N端前B型利钠肽和肌钙蛋白T相似。
血浆HGF是一种有前景的CA筛查工具。CA患者中较高水平的HGF与更严重的HF和更差的预后相关。