Miyake Makito, Yonemoto Naohiro, Togo Kanae, Xu Linghua, Oguri Tomoyo, Tanaka Masayuki, Hasegawa Yoshiyuki, Izawa Yoshinobu, Araki Kenji
Department of Urology, Nara Medical University, Kashihara, Nara, Japan.
Department of Biostatistics, Faculty of Medicine, University of Toyama. Toyama-shi, Toyama, Japan.
JCO Clin Cancer Inform. 2025 Jun;9:e2400249. doi: 10.1200/CCI-24-00249. Epub 2025 Jun 27.
Collecting information on clinical outcomes (recurrence/progression) from complex treatment courses in non-muscle invasive bladder cancer (NMIBC) is challenging and time-consuming. We developed a deep learning natural language processing model to assess outcomes in patients with NMIBC using vast data from electronic health records (EHRs).
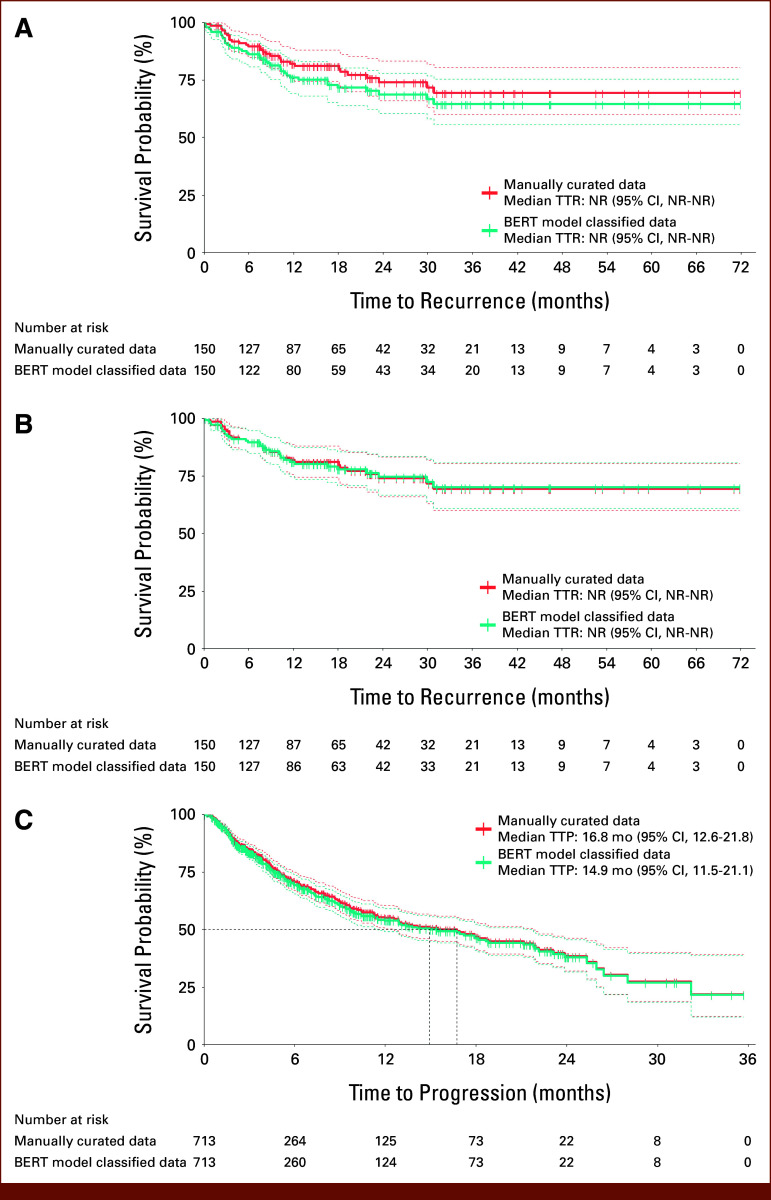
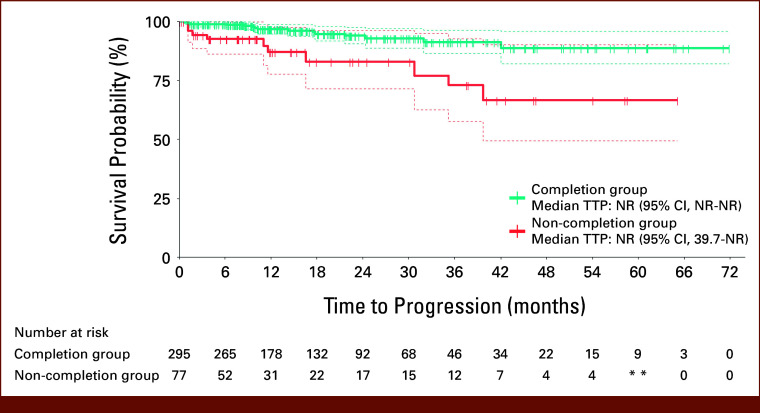
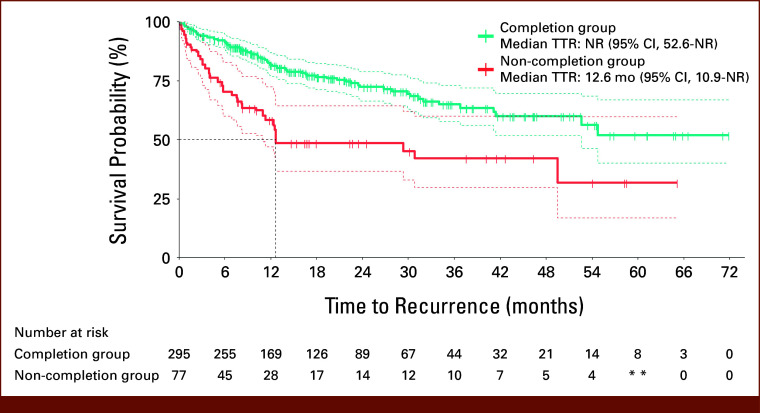
This retrospective study analyzed data from Japanese adults with NMIBC who started Bacillus Calmette-Guérin (BCG) induction therapy between April 2016 and June 2022. A Bidirectional Encoder Representations from Transformers (BERT) model was trained to classify outcomes, supported by human review for past history records. The model's performance was assessed by precision, recall, and F1 scores. We compared the effectiveness of BCG therapy between completion (patients who completed therapy) and non-completion groups.
Of 372 patients studied, 79.3% and 20.7% were in the completion group and the non-completion group, respectively. The final BERT model achieved average F1 scores of 0.91 and 0.98 for time to recurrence (TTR), and 0.74 and 0.94 for time to progression (TTP) before and after human support, respectively. The hazard ratio for TTR in BCG completion versus non-completion groups was 0.40 (95% CI, 0.26 to 0.62) by a multivariate Cox proportional hazard model and 0.41 (95% CI, 0.26 to 0.63) by inverse probability of treatment weighting.
The developed model could compare the clinical outcomes between treatments in patients with NMIBC using EHRs. Human support, although required, was needed in only 10% documents and was deemed feasible. The model was able to demonstrate the difference in TTR and TTP between BCG completion and non-completion groups.
收集非肌层浸润性膀胱癌(NMIBC)复杂治疗过程中的临床结局(复发/进展)信息具有挑战性且耗时。我们开发了一种深度学习自然语言处理模型,以利用电子健康记录(EHR)中的大量数据评估NMIBC患者的结局。
这项回顾性研究分析了2016年4月至2022年6月期间开始接受卡介苗(BCG)诱导治疗的日本成年NMIBC患者的数据。训练了一种基于变换器的双向编码器表征(BERT)模型来对结局进行分类,并由人工审核过往病史记录提供支持。通过精确率、召回率和F1分数评估模型的性能。我们比较了完成治疗组(完成治疗的患者)和未完成治疗组之间BCG治疗的有效性。
在372例研究患者中,分别有79.3%和20.7%属于完成治疗组和未完成治疗组。最终的BERT模型在人工支持前后,复发时间(TTR)的平均F1分数分别为0.91和0.98,进展时间(TTP)的平均F1分数分别为0.74和0.94。多变量Cox比例风险模型显示,BCG完成治疗组与未完成治疗组的TTR风险比为0.40(95%CI,0.26至0.62),治疗权重逆概率法得出的风险比为0.41(95%CI,0.26至0.63)。
所开发的模型能够利用EHR比较NMIBC患者不同治疗之间的临床结局。人工支持虽然是必要的,但仅需审核10%的文档,被认为是可行的。该模型能够证明BCG完成治疗组和未完成治疗组在TTR和TTP方面的差异。