van Hout Denise, Mouncey Paul, Harrison David, Bonten Marc, Derde Lennie, Angus Derek C, Anjum Aisha, Annane Djillali, Best-Lane Janis, Brunkhorst Frank, Cecconi Maurizio, Ehrmann Stephan, Gordon Anthony, Hays Leanne Marie, Kester Esmee, Mahon Niamh, McArthur Colin, Nichol Alistair, Peters Svenja, Pugliese Sara, Rowan Kathryn, Torre-Cisneros Julian, Weis Sebastian
Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht, the Netherlands.
Intensive Care National Audit and Research Centre, London, United Kingdom.
JAMA Netw Open. 2025 Jul 1;8(7):e2518503. doi: 10.1001/jamanetworkopen.2025.18503.
Ethical, administrative, regulatory, and logistical (EARL) procedures can hamper clinical trial delivery. Quantification of these hurdles is rare, prohibiting identification of areas for improvement.
To identify and quantify EARL hurdles in trial delivery before and during the COVID-19 pandemic.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study used data from the ongoing Randomized Embedded Multifactorial Adaptive Platform Trial for Community-Acquired Pneumonia to enable comparison of EARL procedures for multiple protocols across 19 European countries in the pre-COVID-19 pandemic (February 19, 2016 to March 10, 2020) and COVID-19 pandemic (March 11, 2020, to May 4, 2023) periods. Data were analyzed from November 2024 to March 2025 with contracts and protocol submissions as the units of analysis.
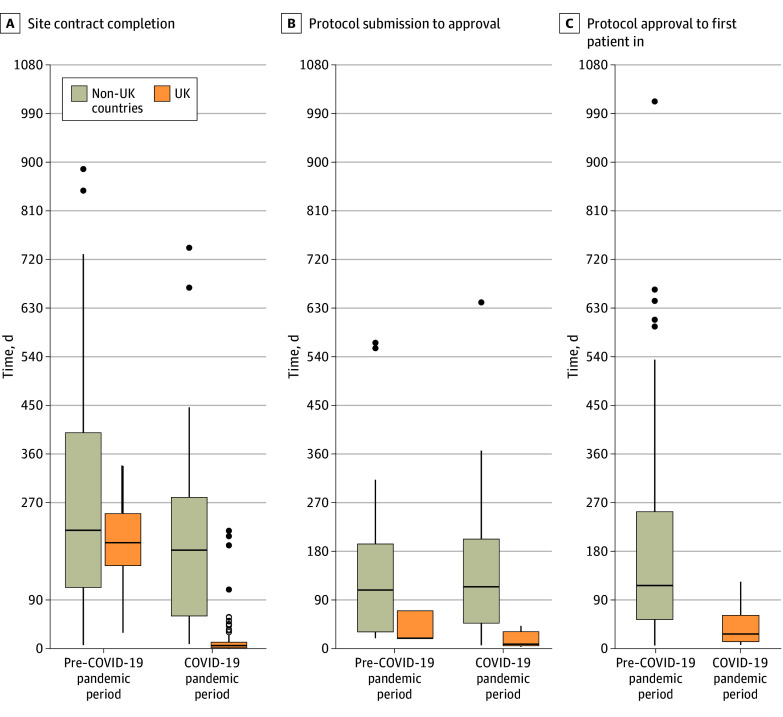
Time to (1) site contract completion, (2) regulatory and ethical approval (TTA), and (3) first patient in (FPI). The UK was compared with non-UK countries because of its distinct research infrastructure.
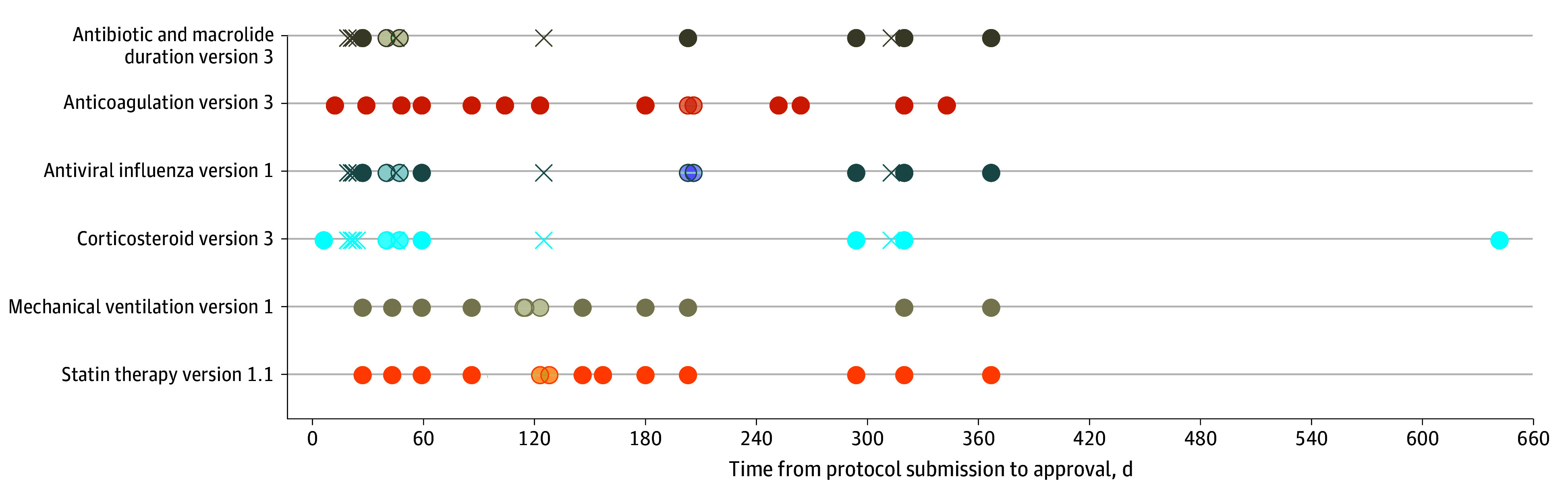
There were 257 fully signed first contracts with study sites for analysis. In the UK, contract completion times decreased by 97% (95% CI, 95% to 98%), from a median (IQR) of 196 (154 to 250) days in the pre-COVID-19 pandemic period to 5 (1 to 11) days during the COVID-19 pandemic. In non-UK countries, median (IQR) contract completion times were 224 (119 to 412) days and 183 (62 to 291) days before and during the COVID-19 pandemic, respectively (relative difference, -18%; 95% CI, -43% to 52%). In total, 44 interventions in 16 domains were submitted, yielding 232 protocol approvals for analysis. During the COVID-19 pandemic, median (IQR) TTA was 8 (5 to 31) days in the UK and 115 (47 to 103) days in non-UK countries (median difference, 107 days; 95% CI, 76 to 123 days), with large variation across non-UK countries. Time between approval and FPI during the COVID-19 pandemic was, on average, 3 months faster in the UK compared with non-UK countries (median difference, 90 days; 95% CI, 42 to 141 days).
This study found that EARL procedures were lengthy and variable between countries, reflecting different interpretations of trial regulations, with faster processes in the UK. These findings underscore the need to streamline processes across European countries to improve trial efficiency, in particular during future public health emergencies such as pandemics.
伦理、行政、监管和后勤(EARL)程序可能会阻碍临床试验的开展。对这些障碍进行量化的情况很少见,这使得难以确定改进的领域。
确定并量化2019冠状病毒病大流行之前和期间试验开展过程中的EARL障碍。
设计、设置和参与者:这项队列研究使用了正在进行的社区获得性肺炎随机嵌入式多因素适应性平台试验的数据,以便比较19个欧洲国家在2019冠状病毒病大流行之前(2016年2月19日至2020年3月10日)和2019冠状病毒病大流行期间(2020年3月11日至2023年5月4日)多个方案的EARL程序。从2024年11月至2025年3月进行数据分析,以合同和方案提交作为分析单位。
(1)研究点合同完成时间、(2)监管和伦理批准时间(TTA)以及(3)首例患者入组时间(FPI)。由于英国有独特的研究基础设施,因此将其与非英国国家进行了比较。
共有257份与研究点的首份合同完全签署用于分析。在英国,合同完成时间减少了97%(95%CI,95%至98%),从2019冠状病毒病大流行之前的中位数(IQR)196(154至250)天降至2019冠状病毒病大流行期间的5(1至11)天。在非英国国家,2019冠状病毒病大流行之前和期间合同完成时间的中位数(IQR)分别为224(119至412)天和183(62至291)天(相对差异为-18%;95%CI,-43%至52%)。总共提交了16个领域的44项干预措施,产生了232项方案批准用于分析。在2019冠状病毒病大流行期间,英国的TTA中位数(IQR)为8(5至31)天,非英国国家为115(47至103)天(中位数差异为107天;95%CI,76至123天),非英国国家之间差异很大。在2019冠状病毒病大流行期间,英国从批准到FPI的时间平均比非英国国家快3个月(中位数差异为90天;95%CI,42至141天)。
本研究发现,EARL程序冗长且各国之间存在差异,反映了对试验法规的不同解释,英国的流程更快。这些发现强调了在欧洲各国简化流程以提高试验效率的必要性,特别是在未来大流行等公共卫生紧急情况期间。