Easwar V Ra Rathina, Navaneethakrishnan R, Agharkar Yogeshwar
Department of Orthopaedics, Sree Balaji Medical College and Hospital, Chennai, Tamil Nadu, India.
J Orthop Case Rep. 2025 Jul;15(7):163-167. doi: 10.13107/jocr.2025.v15.i07.5808.
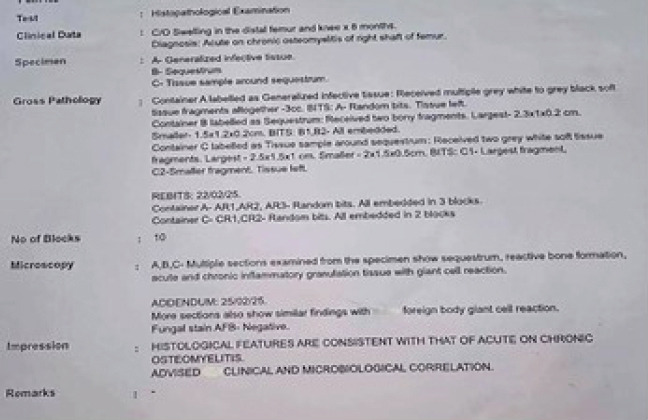
Osteomyelitis is a bone infection that may present acutely or chronically. Acute on chronic osteomyelitis refers to the exacerbation of symptoms in a patient with an underlying chronic infection. This case report presents a 19-year-old male diagnosed with acute on chronic osteomyelitis of the right distal femur, with no history of a discharging sinus for the past 6 months. Osteomyelitis is a bone infection commonly caused by bacteria, with Staphylococcus aureus being the most frequent pathogen. Chronic osteomyelitis can occasionally experience acute flare-ups, referred to as "acute on chronic osteomyelitis". This report discusses the presentation, diagnosis, and management of a 19-year-old male with acute on chronic osteomyelitis of the right distal femur.
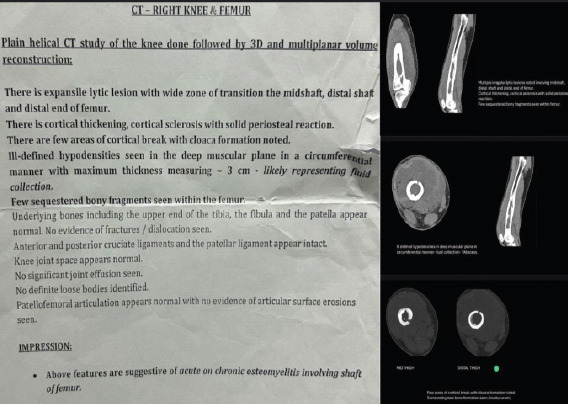
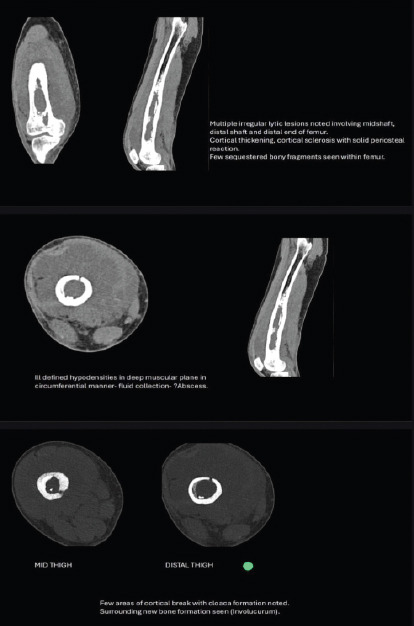
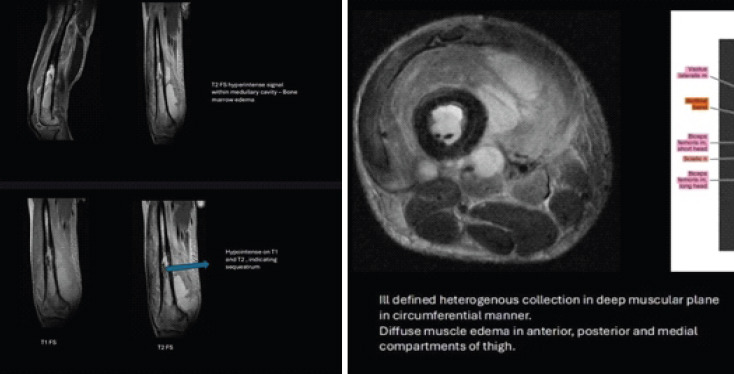
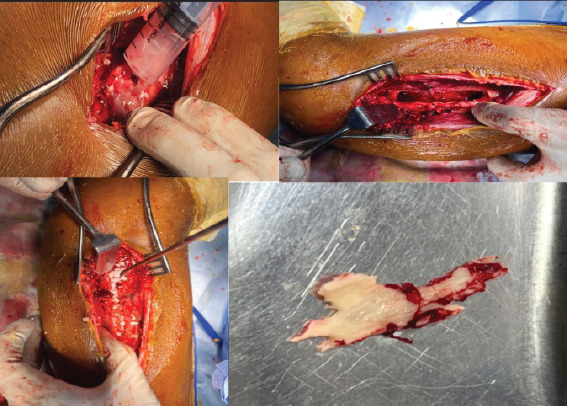
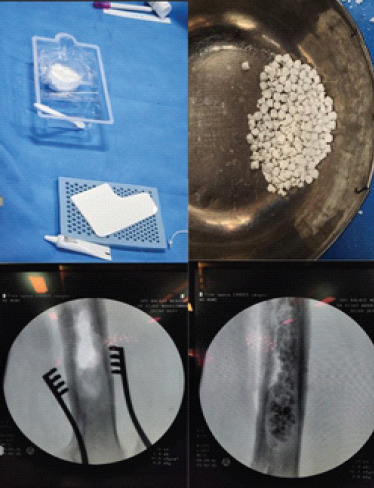
A 19-year-old male presented with increasing pain, swelling, and warmth over his right distal femur for 2 weeks. The pain was deep, throbbing, worsened by weight-bearing, and unrelieved by analgesics. He had similar complaints 6 months ago but had no symptoms such as fever or discharging sinus since then. There was no history of trauma or injury. On physical examination, the patient exhibited localized tenderness, mild swelling, broadening, irregularity, and warmth over the distal femur. Movements of the knee were restricted, and pain was elicited with direct palpation of the femur. No open wounds or discharging sinuses were present, and neurological and vascular examinations were unremarkable.Radiographs of the right femur showed sclerosis and focal cortical thickening, indicating chronic osteomyelitis. Magnetic resonance imaging confirmed the presence of marrow edema, cortical irregularity, and periosteal reaction, supporting the diagnosis of chronic osteomyelitis with an acute exacerbation. Blood tests revealed an elevated white blood cell count and C-reactive protein, indicating an acute inflammatory response. The patient received intravenous antibiotics preoperatively, followed by sequestrectomy, saucerization, and stimulan placement over the site where necrotic bone was removed to promote healing. Over 6 weeks, the patient experienced significant improvement in symptoms. Repeat imaging showed resolution of the acute infection, and long-term oral antibiotics were prescribed to manage chronic osteomyelitis.This case emphasizes the challenges of diagnosing and treating acute on chronic osteomyelitis, particularly when typical signs like a discharging sinus are absent. Early diagnosis and prompt, targeted antibiotic therapy is crucial for preventing complications such as deformities, limb loss, or sepsis.
Effective management of acute on chronic osteomyelitis requires comprehensive evaluation through clinical history, imaging, and laboratory testing. Early intervention with surgical debridement and appropriate antibiotic therapy is vital to achieving favorable outcomes and preventing long-term complications.

骨髓炎是一种可急性或慢性发作的骨感染。慢性骨髓炎急性发作是指潜在慢性感染患者症状的加重。本病例报告介绍了一名19岁男性,被诊断为右股骨远端慢性骨髓炎急性发作,过去6个月无窦道流脓史。骨髓炎是一种常见的由细菌引起的骨感染,金黄色葡萄球菌是最常见的病原体。慢性骨髓炎偶尔会出现急性发作,称为“慢性骨髓炎急性发作”。本报告讨论了一名19岁右股骨远端慢性骨髓炎急性发作男性的临床表现、诊断和治疗。
一名19岁男性,右股骨远端疼痛、肿胀和发热加重2周。疼痛较深,呈搏动性,负重时加重,服用镇痛药不能缓解。6个月前他有类似症状,但此后无发热或窦道流脓等症状。无外伤史。体格检查时,患者右股骨远端有局限性压痛、轻度肿胀、增宽、不规则及发热。膝关节活动受限,直接触诊股骨时诱发疼痛。无开放性伤口或窦道流脓,神经和血管检查无异常。右股骨X线片显示骨质硬化和局部皮质增厚,提示慢性骨髓炎。磁共振成像证实存在骨髓水肿、皮质不规则和骨膜反应,支持慢性骨髓炎急性加重的诊断。血液检查显示白细胞计数和C反应蛋白升高,提示急性炎症反应。患者术前接受静脉抗生素治疗,随后进行死骨切除术、碟形手术,并在去除坏死骨的部位放置刺激物以促进愈合。6周内,患者症状明显改善。复查影像学显示急性感染消退,开具长期口服抗生素治疗慢性骨髓炎。本病例强调了诊断和治疗慢性骨髓炎急性发作的挑战,尤其是在没有窦道流脓等典型体征时。早期诊断和及时、有针对性的抗生素治疗对于预防畸形、肢体缺失或败血症等并发症至关重要。
慢性骨髓炎急性发作的有效管理需要通过临床病史、影像学和实验室检查进行全面评估。早期进行手术清创和适当的抗生素治疗对于取得良好疗效和预防长期并发症至关重要。