Cao Yuan, Li Xiuzhi, Cui Zengzhen, Lv Yang, Si Gao
Department of Orthopedics, Peking University Third Hospital, Beijing, China.
Engineering Research Center of Bone and Joint Precision Medicine, Beijing, China.
J Orthop Surg Res. 2025 Jul 12;20(1):647. doi: 10.1186/s13018-025-06019-0.
Acute Achilles tendon rupture (AATR) surgical repair debates center on the clinical efficacy of minimally invasive surgery (MIS) versus open surgery (OS), with immobilization duration poorly stratified. This prospective cohort study aimed to compare clinical outcomes of OS and MIS for AATR repair and evaluate the impact of immobilization duration (0, 2, or 4 weeks) on postoperative rehabilitation.
A total of 474 patients undergoing surgical repair for acute AATR were stratified into six groups based on surgical approach (OS: 265 cases; MIS: 209 cases) and immobilization duration (0, 2, or 4 weeks). The primary outcomes were postoperative complications, while secondary outcomes included recovery times for Achilles tendon function. Data regarding the operative times, incision lengths, the visual analog scale (VAS) score, the Achilles tendon Total Rupture Score (ATRS), and the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Scale score, and the relative Achilles tendon resting angle (ATRA) were also collected.
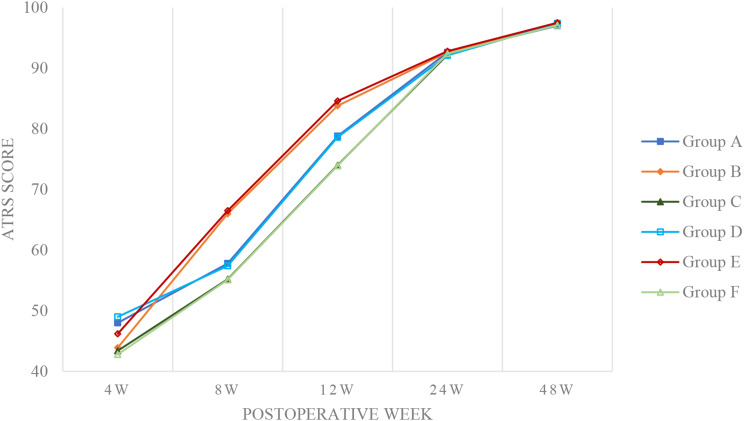
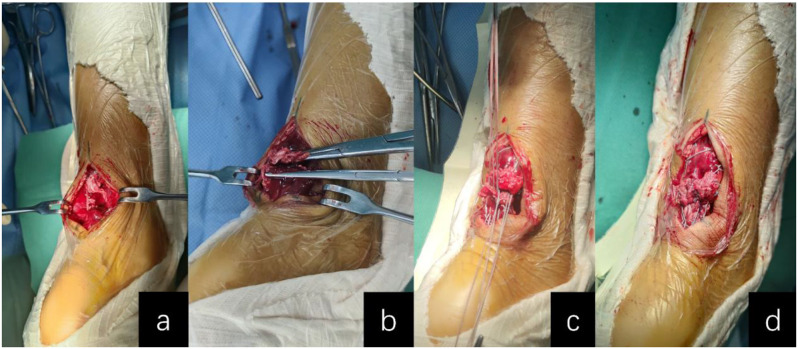
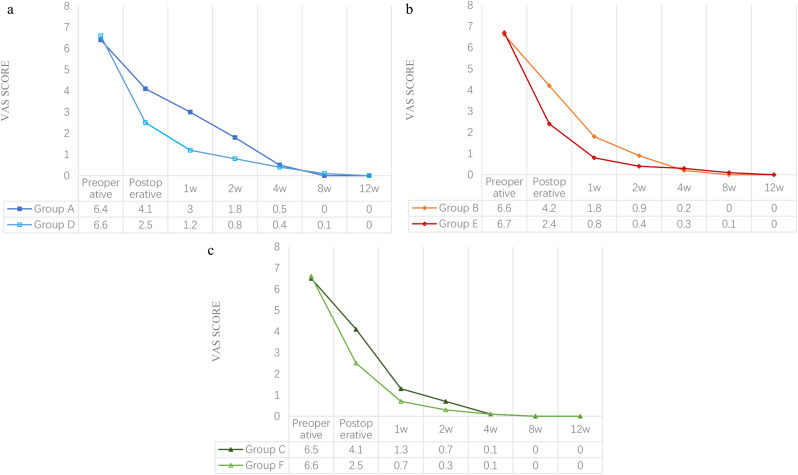
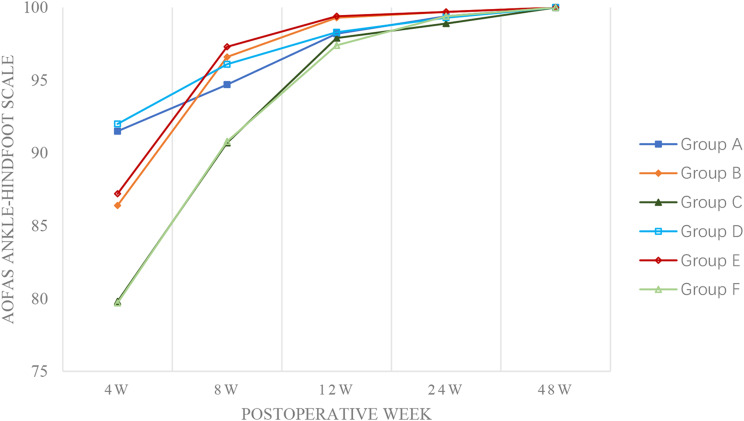
MIS groups demonstrated significantly shorter operative times (34.1-34.4 vs. 45.1-46.1 min, P < 0.001) and reduced incision lengths (2.2-2.4 vs. 4.5-4.7 cm, P < 0.001) compared to OS. Postoperative VAS scores were markedly lower in MIS cohorts during the first 2 weeks (P < 0.001), with pain resolution comparable across all groups by 8 weeks. Despite the superior early functional recovery in PF (9.1-33.4 vs. 14.6-38.9 days, P < 0.001), Group D and E exhibited higher re-injury rates compared to OS (P < 0.05), in which Group D also demonstrated higher re-operation rates (5.6% vs. 0, P = 0.038). Prolonged immobilization (4 weeks) delayed functional recovery in both cohorts (P < 0.001). While transient differences in AOFAS Ankle-Hindfoot Scale and ATRS scores were observed at intermediate time points, all groups achieved near-maximal functional scores by 48 weeks, with no significant between-group differences (P > 0.05). Relative ATRA exhibited no significant intergroup differences at 48 weeks postoperatively (P > 0.05).
MIS for acute Achilles tendon rupture achieves faster early recovery but carries higher re-injury risks, mitigated by 4-week immobilization. OS benefits from shorter (2-week) immobilization. Both approaches yield equivalent long-term functions, emphasizing the need for tailored protocols and refined MIS techniques to optimize outcomes.
NCT04663542.
急性跟腱断裂(AATR)手术修复的争论主要集中在微创手术(MIS)与开放手术(OS)的临床疗效上,而固定时间的分层并不完善。这项前瞻性队列研究旨在比较AATR修复中OS和MIS的临床结果,并评估固定时间(0、2或4周)对术后康复的影响。
共有474例接受急性AATR手术修复的患者根据手术方式(OS:265例;MIS:209例)和固定时间(0、2或4周)分为六组。主要结局是术后并发症,次要结局包括跟腱功能的恢复时间。还收集了手术时间、切口长度、视觉模拟量表(VAS)评分、跟腱完全断裂评分(ATRS)、美国矫形足踝协会(AOFAS)踝-后足量表评分以及相对跟腱静息角(ATRA)的数据。
与OS相比,MIS组的手术时间明显更短(34.1 - 34.4分钟对45.1 - 46.1分钟,P < 0.001),切口长度也更短(2.2 - 2.4厘米对4.5 - 4.7厘米,P < 0.001)。在术后前2周,MIS队列的VAS评分明显更低(P < 0.001),到8周时所有组的疼痛缓解情况相当。尽管PF组早期功能恢复更好(9.1 - 33.4天对14.6 - 38.9天,P < 0.001),但D组和E组的再损伤率高于OS组(P < 0.05),其中D组的再次手术率也更高(5.6%对0,P = 0.038)。延长固定时间(4周)会延迟两个队列的功能恢复(P < 0.001)。虽然在中间时间点观察到AOFAS踝-后足量表和ATRS评分存在短暂差异,但所有组在48周时均达到接近最大功能评分,组间无显著差异(P > 0.05)。术后48周时相对ATRA组间无显著差异(P > 0.05)。
急性跟腱断裂的MIS可实现更快的早期恢复,但再损伤风险更高,4周固定可减轻这种风险。OS受益于更短(2周)的固定。两种方法产生的长期功能相当,强调需要制定个性化方案并改进MIS技术以优化结果。
NCT04663542。