Barclay Matthew E, McPhail Sean, Johnson Shane A, Swann Ruth, Finley Christian J, Butler John, Alvi Riaz, Barisic Andriana, Bennett Damien B, Bucher Oliver, Creighton Nicola, Denny Cheryl A, Dewar Ron A, Donnelly David W, Dowden Jeff J, Downie Laura, Finn Norah, Habbous Steven, Huws Dyfed W, Kumar S Eshwar, May Leon, McClure Carol A, Møller Bjørn, Morrison David S, Musto Grace, Nilssen Yngvar, Saint-Jacques Nathalie, Sarker Sabuj, Shack Lorraine, Te Marvelde Luc, Tian Xiaoyi, Thomas Robert Js, Thomson Catherine S, Walton Richard, Wang Haiyan, Wong Tommy Hon Ting, Woods Ryan R, You Hui, Zhang Bin, Lyratzopoulos Georgios
Epidemiology of Cancer Healthcare & Outcomes (ECHO), Department of Behavioural Science & Health, Institute of Epidemiology & Health Care (IEHC), UCL, London, UK.
National Disease Registration Service, NHS England, Leeds, UK.
BMJ Oncol. 2025 Jul 11;4(1):e000800. doi: 10.1136/bmjonc-2025-000800. eCollection 2025.
International variation in lung cancer survival may be partly explained by variation in stage-specific treatment use, but relevant comparative evidence is sparse. As part of the International Cancer Benchmarking Partnership, we examined use of chemotherapy and radiotherapy in population-based cancer registry data.
Linked population-based data sources were used to describe use and time to first treatment for either chemotherapy or radiotherapy in patients with lung cancer diagnosed in study periods during 2012-2017 in 16 jurisdictions of Australia, Canada, the UK and Norway.
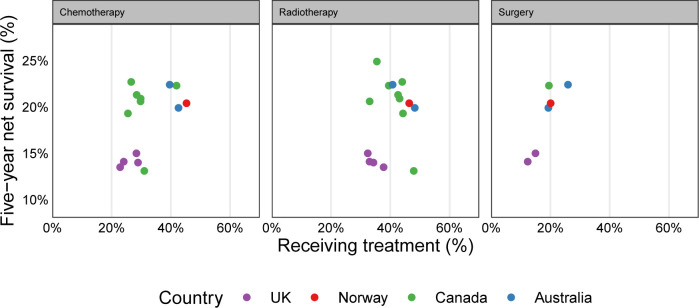
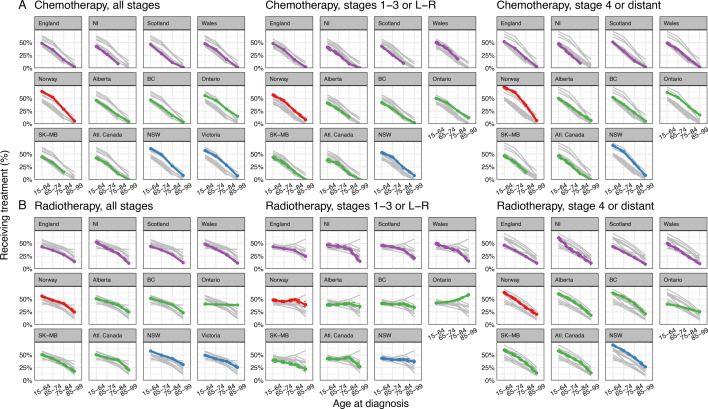
There was large variation in the proportions of patients with lung cancer receiving chemotherapy (ranging from 23% in Northern Ireland to 45% in Norway) and radiotherapy (ranging from 32% in England to 48% in New South Wales and 50% in Newfoundland and Labrador). Across jurisdictions, chemotherapy use decreased steeply with increasing age, regardless of stage at diagnosis. For radiotherapy use, in stage 1-3 cancer three patterns were observed: (a) steep decrease with increasing age (UK jurisdictions, Saskatchewan-Manitoba); (b) a relatively flat pattern (Norway, Alberta, British Columbia, Atlantic Canada, New South Wales) and (c) increasing use with increasing age (Ontario).Time to radiotherapy initiation was longer in the UK jurisdictions than elsewhere; time to chemotherapy was longer in the UK and Canadian jurisdictions except Ontario.
Use of chemotherapy and radiotherapy in patients with lung cancer varied substantially between jurisdictions during the mid-2010s within age-stage strata. Reasons for these variations are unclear. Differences in non-surgical treatment use are plausibly associated with international variation in lung cancer survival.
肺癌生存率的国际差异可能部分归因于特定分期治疗方法使用上的差异,但相关的比较证据较少。作为国际癌症基准化伙伴关系的一部分,我们在基于人群的癌症登记数据中研究了化疗和放疗的使用情况。
利用基于人群的关联数据源,描述了2012年至2017年研究期间在澳大利亚、加拿大、英国和挪威的16个司法管辖区诊断出的肺癌患者接受化疗或放疗的使用情况及首次治疗时间。
肺癌患者接受化疗的比例差异很大(从北爱尔兰的23%到挪威的45%),接受放疗的比例也差异很大(从英格兰的32%到新南威尔士的48%以及纽芬兰和拉布拉多的50%)。在各个司法管辖区,无论诊断时处于何阶段,化疗的使用都随着年龄的增长而急剧下降。对于放疗的使用,在1 - 3期癌症中观察到三种模式:(a) 随着年龄增长急剧下降(英国各司法管辖区、萨斯喀彻温省 - 曼尼托巴省);(b) 相对平稳的模式(挪威、艾伯塔省、不列颠哥伦比亚省、加拿大大西洋省份、新南威尔士);(c) 随着年龄增长使用增加(安大略省)。在英国各司法管辖区,开始放疗的时间比其他地方更长;在英国和加拿大各司法管辖区(安大略省除外),开始化疗的时间更长。
在2010年代中期,年龄 - 分期分层内,各司法管辖区肺癌患者化疗和放疗的使用情况差异很大。这些差异的原因尚不清楚。非手术治疗使用上的差异可能与肺癌生存率的国际差异有关。