Regmi Dhiraj R, Kshetri Sandeep, Wagle Laxman, Regmi Sabita
Internal Medicine, Nepalese Army Institute of Health Sciences, Kathmandu, NPL.
Internal Medicine, MedStar Franklin Square Medical Center, Baltimore, USA.
Cureus. 2025 Jun 14;17(6):e86024. doi: 10.7759/cureus.86024. eCollection 2025 Jun.
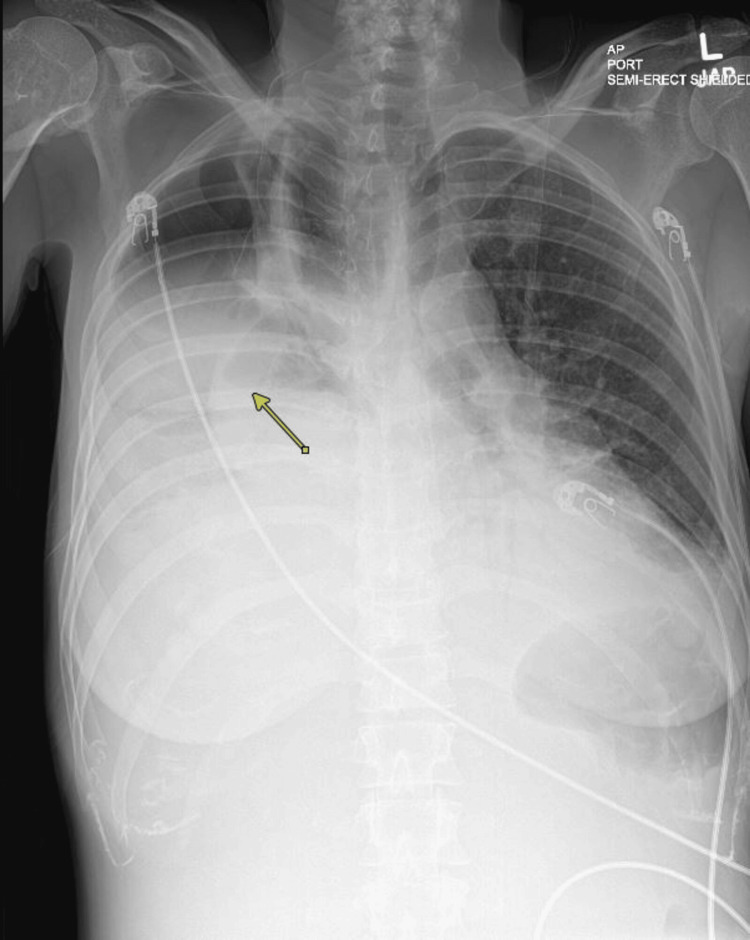
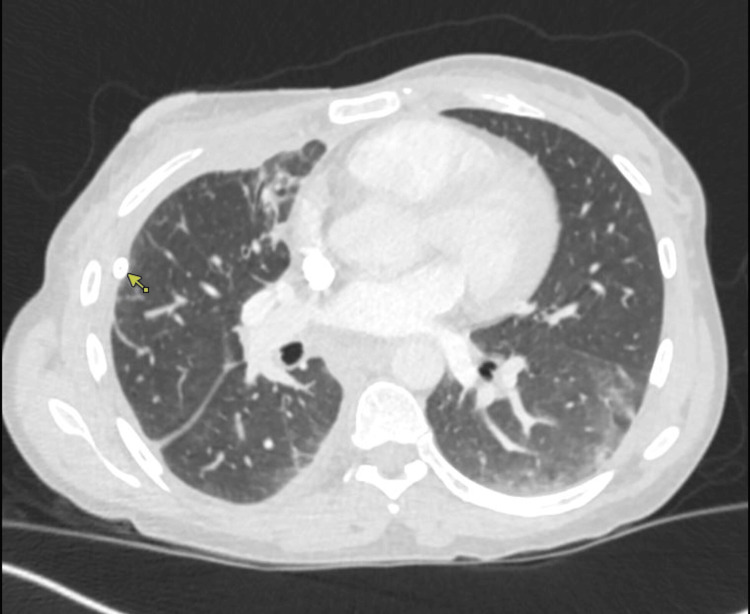
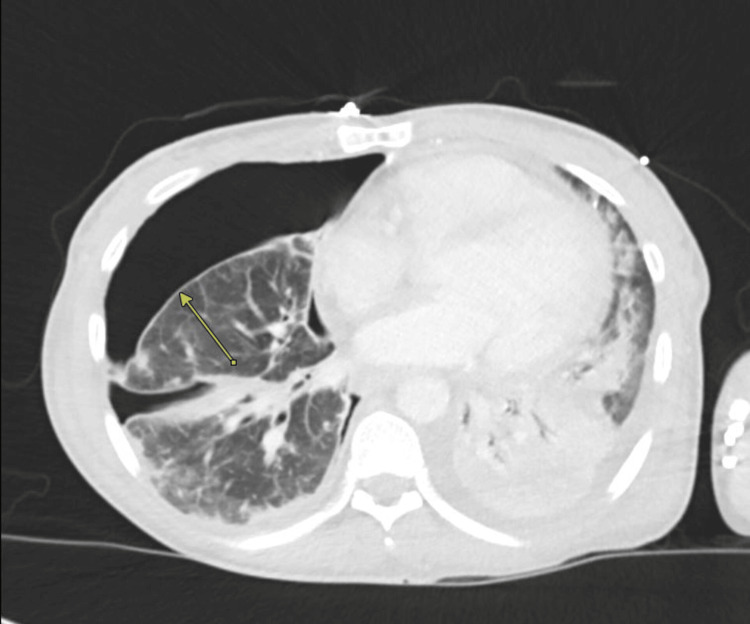
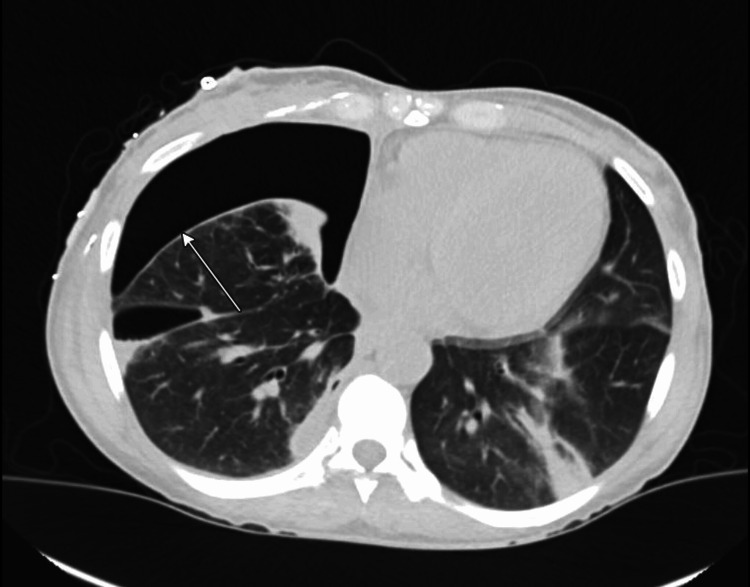
Empyema is a rare but serious complication in patients with COVID-19, and its association with bronchopleural fistula (BPF) is even more uncommon. We present the case of a 40-year-old woman with a history of intravenous drug use who developed polymicrobial empyema in the setting of COVID-19, further complicated by BPF. She presented with hypoxic respiratory failure, leukocytosis, and lactic acidosis. Imaging revealed a large right-sided hydropneumothorax and bilateral lung opacities. Broad-spectrum antibiotics, antivirals, and corticosteroids were initiated, and 3 liters of purulent fluid were drained via chest tube, confirming empyema. Cultures identified multiple pathogens, including , , methicillin-sensitive , and Group C/G streptococci. Persistent air leak and incomplete lung re-expansion led to a diagnosis of BPF. The patient was successfully managed with prolonged antibiotic therapy and chest tube drainage without requiring surgical or bronchoscopic intervention. This case highlights the importance of recognizing and conservatively managing small BPFs in COVID-19-associated empyema, emphasizing the potential for non-surgical resolution in select cases.
脓胸是新冠肺炎患者中一种罕见但严重的并发症,其与支气管胸膜瘘(BPF)的关联更为罕见。我们报告一例40岁有静脉吸毒史的女性,在新冠肺炎背景下发生了多微生物脓胸,并进一步并发BPF。她表现为低氧性呼吸衰竭、白细胞增多和乳酸酸中毒。影像学检查显示右侧大量液气胸和双侧肺部混浊。开始使用广谱抗生素、抗病毒药物和皮质类固醇,通过胸腔引流管引流了3升脓性液体,确诊为脓胸。培养物鉴定出多种病原体,包括 、 、甲氧西林敏感 以及C/G组链球菌。持续的气胸漏气和肺不完全复张导致BPF的诊断。该患者通过延长抗生素治疗和胸腔引流管引流成功得到治疗,无需手术或支气管镜干预。该病例强调了在新冠肺炎相关脓胸中识别和保守处理小BPF的重要性,强调了部分病例非手术解决的可能性。