Placik Daniel A, Taylor Wesley L, Wnuk Nathan M
Yuma Regional Medical Center, 2500 South 8th Avenue, Suite 200, Yuma, AZ, 85364.
Yuma Regional Medical Center, Department of Interventional Radiology, Yuma, AZ.
Radiol Case Rep. 2020 Nov;15(11):2378-2381. doi: 10.1016/j.radcr.2020.09.026. Epub 2020 Sep 18.
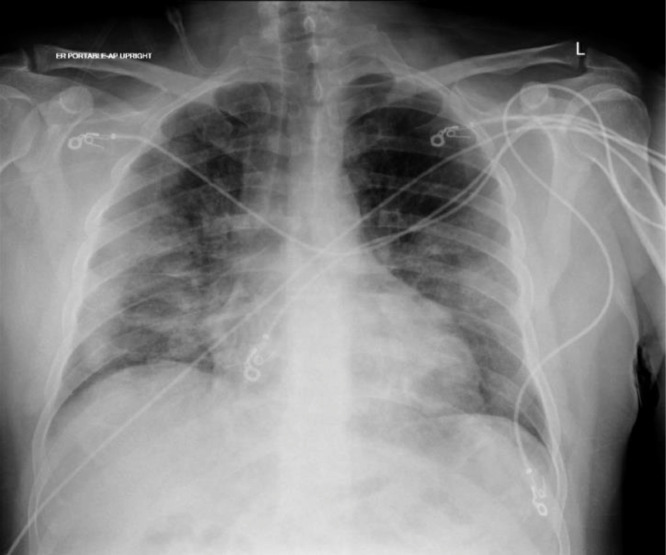
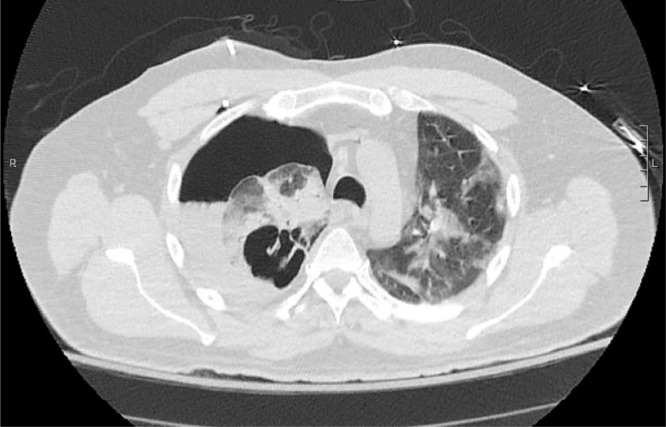
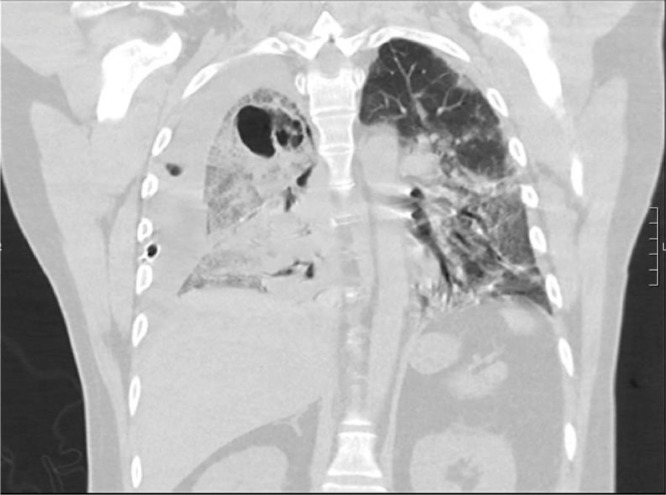
COVID-19 pneumonia has demonstrated a wide spectrum of clinical presentations that has yet to be completely uncovered. We discuss the case of a 49-year-old male who presented to the emergency department with fever, cough, and shortness of breath. Initial chest X-ray suggested viral pneumonia that was confirmed to be due to COVID-19. He was treated with empiric antibiotics, antiviral therapy, high-dose glucocorticoids, and interleukin antagonists. Two weeks into the patient's hospital course, he rapidly decompensated with subsequent chest X-ray and CT chest confirming tension pneumothorax with bronchopleural fistula. Intraoperative samples of the necrotic empyema identified mucormycosis invading the lung parenchyma with follow-up microbiology results confirming Rhizopus species. In this case report, we explore the possibility that the patient's immunocompromised state may have contributed to the patient's development of mucormycosis and subsequent development of bronchopleural fistula.
新型冠状病毒肺炎(COVID-19肺炎)已呈现出一系列尚未完全揭示的临床表现。我们讨论了一名49岁男性的病例,该患者因发热、咳嗽和呼吸急促就诊于急诊科。初始胸部X线检查提示为病毒性肺炎,后确诊为COVID-19所致。他接受了经验性抗生素、抗病毒治疗、大剂量糖皮质激素和白细胞介素拮抗剂治疗。在患者住院病程的两周时,他迅速病情恶化,随后的胸部X线和胸部CT证实为张力性气胸伴支气管胸膜瘘。术中坏死性脓胸样本鉴定出毛霉菌病侵犯肺实质,后续微生物学结果证实为根霉菌属。在本病例报告中,我们探讨了患者免疫功能低下状态可能导致其发生毛霉菌病以及随后出现支气管胸膜瘘的可能性。