Wei Jingjing, Wang Aolong, Yu Peng, Sun Yang, Wu Wenjun, Zhang Yilin, Yu Rui, Li Bin, Zhu Mingjun
Department of Cardiovascular Disease, The First Affiliated Hospital of Henan University of Chinese Medicine, Renmin Road 19, Jinshui District, Zhengzhou, 450000, China.
Department of Orthopedics, The First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, 450000, Henan, China.
Chin Med. 2025 Jul 17;20(1):93. doi: 10.1186/s13020-025-01151-9.
Ischemic heart failure (IHF) is a multifaceted syndrome associated with significant mortality and high hospitalization rates globally. According to traditional Chinese medicine (TCM) theory, Qi Deficiency and Blood Stasis (QXXY) Syndrome serves as the pathological basis of IHF. This study aims to investigate the biological basis of QXXY syndrome in IHF patients through an integrated multi-omics approach.
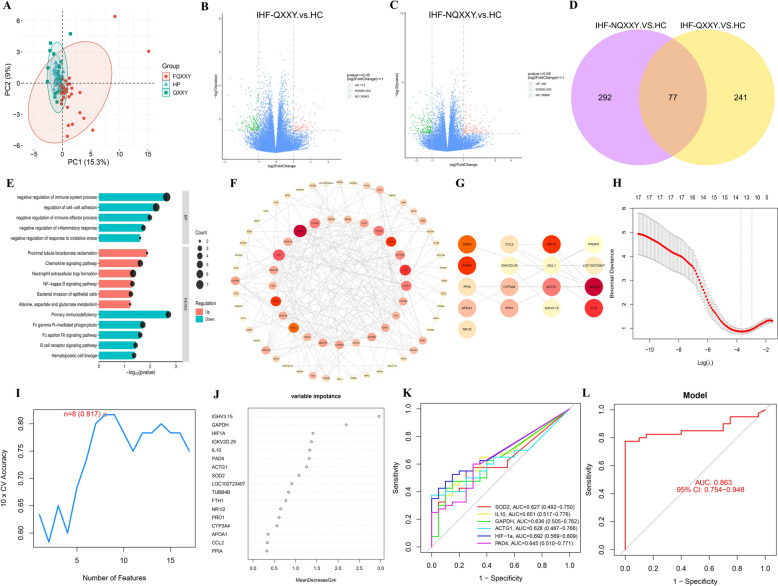
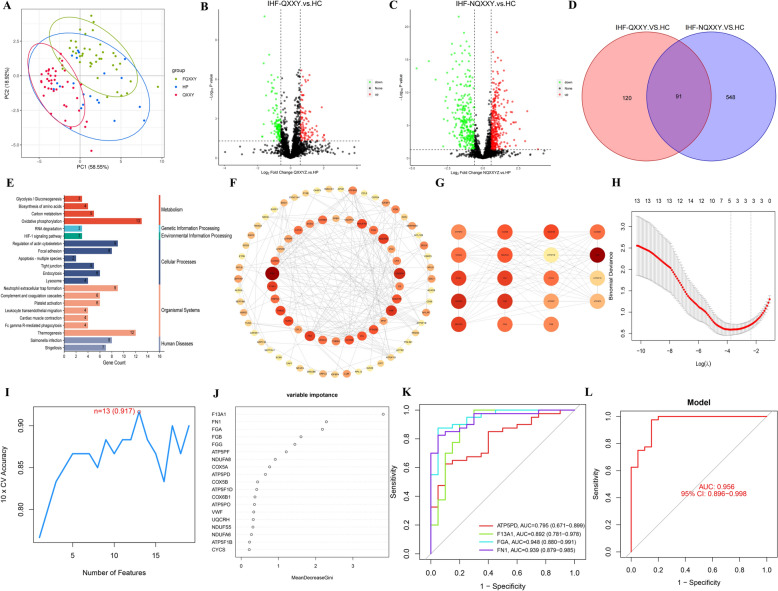
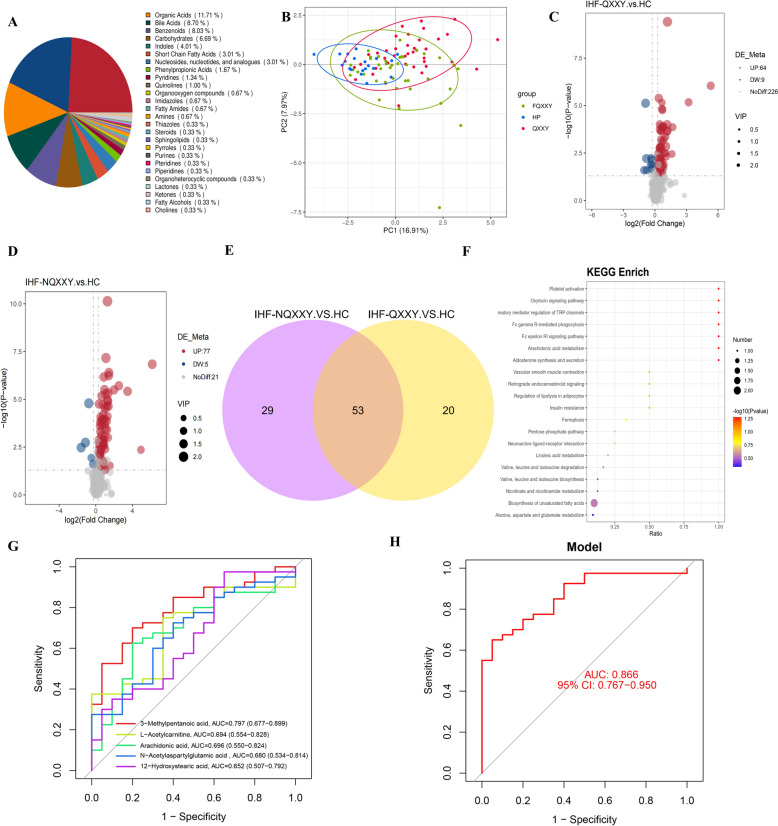
We enrolled 100 participants, comprising 40 IHF patients with QXXY syndrome (IHF-QXXY), 40 IHF patients without QXXY syndrome, and 20 healthy controls. Utilizing an integrated approach combining RNA sequencing (RNA-seq), data-independent acquisition (DIA) proteomics, and targeted metabolomics, we established a comprehensive "gene-protein-metabolite" network for IHF-QXXY syndrome. Candidate biomarkers were identified through machine learning algorithms and further validated using RT-qPCR and targeted proteomics via intelligent parallel reaction monitoring (iPRM).
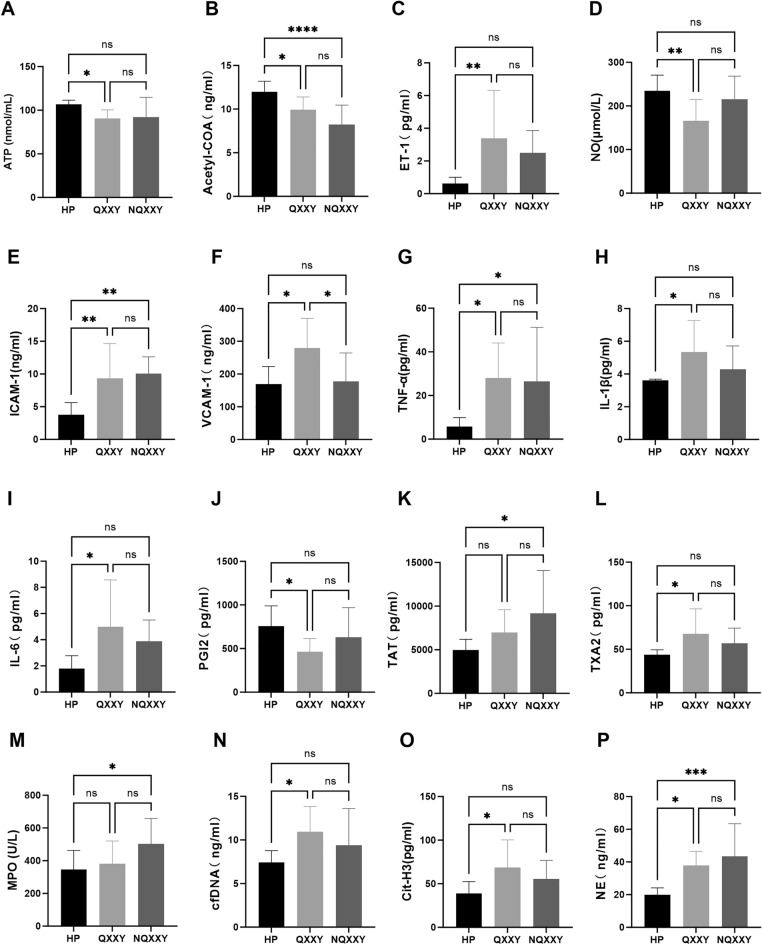
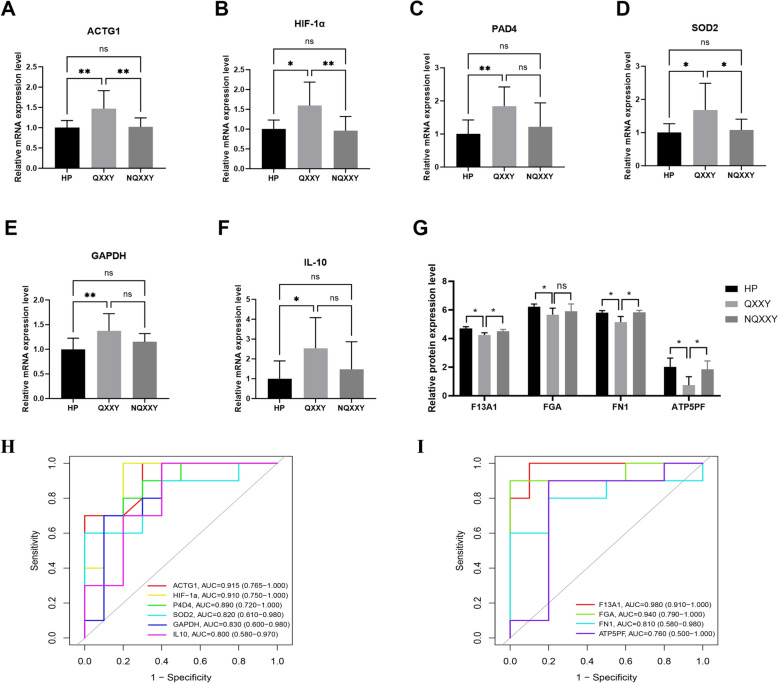
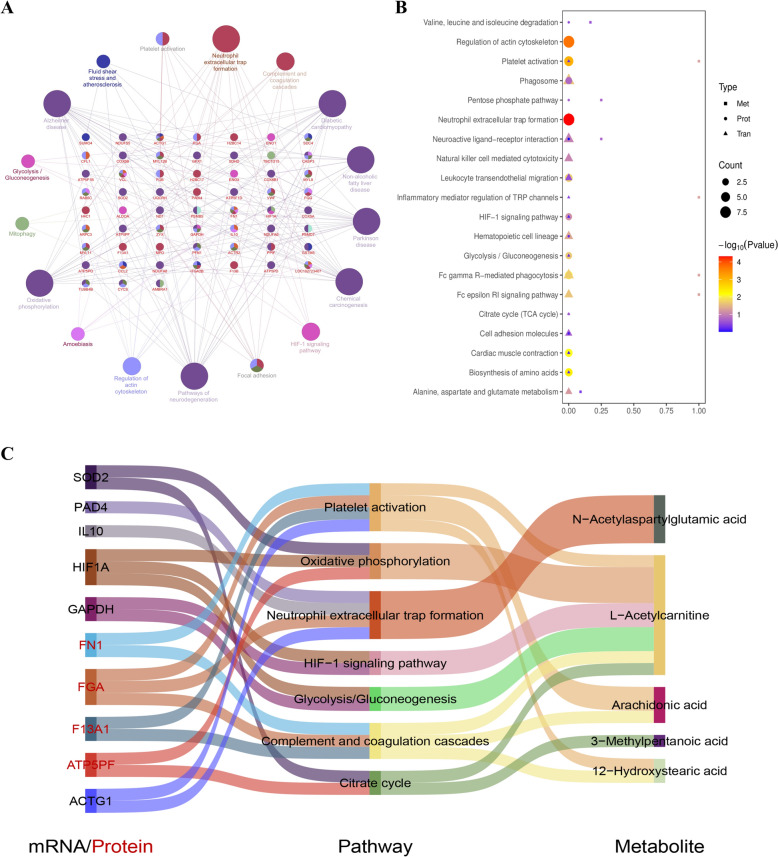
Patients with IHF-QXXY syndrome present with pronounced disruptions in energy metabolism, chronic inflammation, and coagulation abnormalities. The "gene-protein-metabolite" network of IHF-QXXY syndrome comprises six mRNAs, four proteins, and five metabolites. Key pathways involve the activation of neutrophil extracellular traps formation, platelet activation, the HIF-1 signaling pathway, and glycolysis/gluconeogenesis, alongside the suppression of the citrate cycle and oxidative phosphorylation. The key metabolites potentially associated with QXXY syndrome include 3-methylpentanoic acid, arachidonic acid, N-acetylaspartylglutamic acid, L-acetylcarnitine, and 12-hydroxystearic acid. We identified a panel of candidate biomarkers, including HIF-1α, IL10, PAD4, ACTG1, SOD2, GAPDH, FGA, FN1, F13A1, and ATP5PF. This biomarker combination significantly enhanced the diagnostic performance of IHF-QXXY syndrome (AUC > 0.863) and retained high diagnostic accuracy during validation (AUC > 0.75).
This study provides a comprehensive characterization of the molecular features of QXXY syndrome in IHF patients, highlighting key pathways and biomarkers linked to energy metabolism dysregulation, chronic inflammation, and coagulation abnormalities. These findings may provide novel insights and methods for further advancing this research field.
缺血性心力衰竭(IHF)是一种多方面的综合征,在全球范围内与显著的死亡率和高住院率相关。根据中医理论,气虚血瘀(QXXY)证是缺血性心力衰竭的病理基础。本研究旨在通过综合多组学方法探讨缺血性心力衰竭患者QXXY证的生物学基础。
我们招募了100名参与者,包括40例患有QXXY证的缺血性心力衰竭患者(IHF-QXXY)、40例无QXXY证的缺血性心力衰竭患者和20名健康对照。利用RNA测序(RNA-seq)、数据非依赖采集(DIA)蛋白质组学和靶向代谢组学相结合的综合方法,我们建立了一个针对IHF-QXXY证的全面的“基因-蛋白质-代谢物”网络。通过机器学习算法鉴定候选生物标志物,并使用RT-qPCR和通过智能平行反应监测(iPRM)的靶向蛋白质组学进一步验证。
IHF-QXXY证患者存在能量代谢明显紊乱、慢性炎症和凝血异常。IHF-QXXY证的“基因-蛋白质-代谢物”网络由6种mRNA、4种蛋白质和5种代谢物组成。关键途径包括中性粒细胞胞外陷阱形成的激活、血小板激活、HIF-1信号通路和糖酵解/糖异生,同时伴有柠檬酸循环和氧化磷酸化的抑制。可能与QXXY证相关的关键代谢物包括3-甲基戊酸、花生四烯酸、N-乙酰天冬氨酰谷氨酸、L-乙酰肉碱和12-羟基硬脂酸。我们鉴定了一组候选生物标志物,包括HIF-1α、IL10、PAD4、ACTG1、SOD2、GAPDH、FGA、FN1、F13A1和ATP5PF。这种生物标志物组合显著提高了IHF-QXXY证的诊断性能(AUC>0.863),并在验证过程中保持了较高的诊断准确性(AUC>0.75)。
本研究全面描述了缺血性心力衰竭患者QXXY证的分子特征,突出了与能量代谢失调、慢性炎症和凝血异常相关的关键途径和生物标志物。这些发现可能为进一步推进该研究领域提供新的见解和方法。