Brijmohan Sharmela, Mullally Jamie A
Westchester Medical Center. Endocrinology, Diabetes and Metabolism, School of Medicine, New York Medical College, Valhalla, New York.
AACE Endocrinol Diabetes. 2025 Apr 10;12(1):30-33. doi: 10.1016/j.aed.2025.03.004. eCollection 2025 May-Jun.
BACKGROUND/OBJECTIVE: Hypothalamic obesity (HO) is a rare but severe form of obesity characterized by hypothalamic damage resulting in hyperphagia and decreased energy expenditure. Tumors involving the hypothalamus, most commonly craniopharyngiomas, frequently result in HO. Treatment is typically refractory to standard antiobesity treatment modalities. Herein, we describe a young man with HO due to surgical resection of a large craniopharyngioma who was successfully treated with tirzepatide, a novel treatment for obesity and type 2 diabetes.
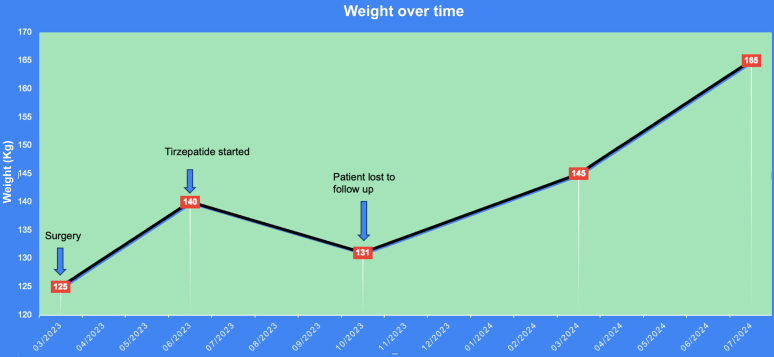
A 21-year-old man presented with headaches for 7 months. His physical examination revealed a body weight of 125 kg (body mass index [BMI], 35 kg/m). Brain magnetic resonance imaging revealed a 5-cm multicystic lobulated sellar mass with suprasellar extension. He underwent transsphenoidal resection, and pathology revealed craniopharyngioma. Postoperatively, he developed hyperphagia and rapid weight gain of 15 kg over 3 months (weight, 140 kg; BMI, 40 kg/m). He was started on tirzepatide, which was gradually up titrated to 10 mg in the first 4 months, during which time he lost 9 kg (weight, 131 kg; BMI, 37 kg/m).
The pathophysiology of HO is complex, involving decreased sympathetic activity and energy expenditure, central insulin and leptin resistance, and increased energy storage in adipose tissue. By modulating sympathetic/parasympathetic tone and regulating energy balance, tirzepatide appears to be a promising agent to address the complex pathophysiology of HO.
This case report highlights the novel use of tirzepatide in the treatment of HO. This case informs clinicians of the potential benefits of considering tirzepatide in the management of HO and encourages further exploration of its use in this context.
背景/目的:下丘脑性肥胖(HO)是一种罕见但严重的肥胖形式,其特征是下丘脑受损,导致食欲亢进和能量消耗减少。累及下丘脑的肿瘤,最常见的是颅咽管瘤,常导致HO。标准的抗肥胖治疗方式通常对其治疗无效。在此,我们描述一名因大型颅咽管瘤手术切除导致HO的年轻男性,他成功接受了替尔泊肽治疗,替尔泊肽是一种用于治疗肥胖症和2型糖尿病的新型药物。
一名21岁男性因头痛7个月就诊。体格检查显示体重125千克(体重指数[BMI],35千克/平方米)。脑部磁共振成像显示一个5厘米的多房分叶状鞍区肿物并向上延伸至鞍上。他接受了经蝶窦切除术,病理显示为颅咽管瘤。术后,他出现食欲亢进,3个月内体重迅速增加15千克(体重140千克;BMI,40千克/平方米)。他开始使用替尔泊肽,在最初4个月内逐渐滴定至10毫克,在此期间他体重减轻了9千克(体重131千克;BMI,37千克/平方米)。
HO的病理生理学很复杂,涉及交感神经活动和能量消耗减少、中枢胰岛素和瘦素抵抗以及脂肪组织中能量储存增加。通过调节交感/副交感神经张力和调节能量平衡,替尔泊肽似乎是一种有前途的药物,可应对HO复杂的病理生理学。
本病例报告突出了替尔泊肽在HO治疗中的新用途。该病例告知临床医生在HO管理中考虑替尔泊肽的潜在益处,并鼓励在此背景下进一步探索其用途。