Raat Willem, Smeets Miek, Van Pottelbergh Gijs, Van de Putte Marie, Janssens Stefan, Vaes Bert
Department of Public Health and Primary Care, KU Leuven, Leuven, Flanders, Belgium
Department of Family Medicine and Population Health, Universiteit Antwerpen, Antwerpen, Belgium.
BMJ Open. 2025 Jul 20;15(7):e093414. doi: 10.1136/bmjopen-2024-093414.
Heart failure is an important health problem and patients are generally older with several comorbidities. Multidisciplinary heart failure care is therefore recommended. However, there is little evidence in real-world settings on how to involve primary care health professionals and how to evaluate such programmes. The main objective of this study is to integrate and evaluate several disease management interventions in a primary care setting.
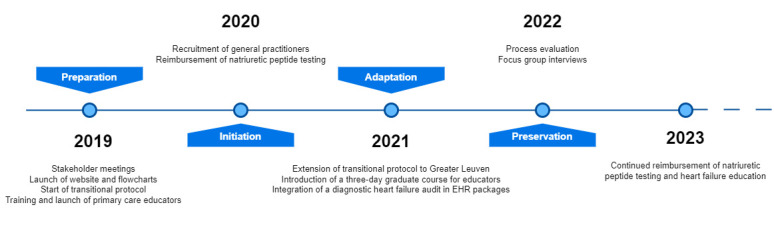
Prospective, non-randomised, observational implementation study with a mixed-methods process evaluation conducted over 3 years (2020-2022).
Primary care practices and two regional hospitals (one tertiary, one secondary) in the Leuven region, Belgium, serving approximately 100 000 inhabitants.
100 general practitioners (GPs) from 19 practices participated. A total of 96 patients were included in the disease management programme. Inclusion criteria for patients included high-risk status for heart failure (HF) readmission, based on clinical criteria. Exclusion criteria were not explicitly defined but participation required informed consent.
Four interventions were implemented: (1) online HF education for GPs, (2) reimbursed natriuretic peptide (NP) testing, (3) patient education by trained primary care HF educators and (4) a structured transitional care protocol posthospital discharge.
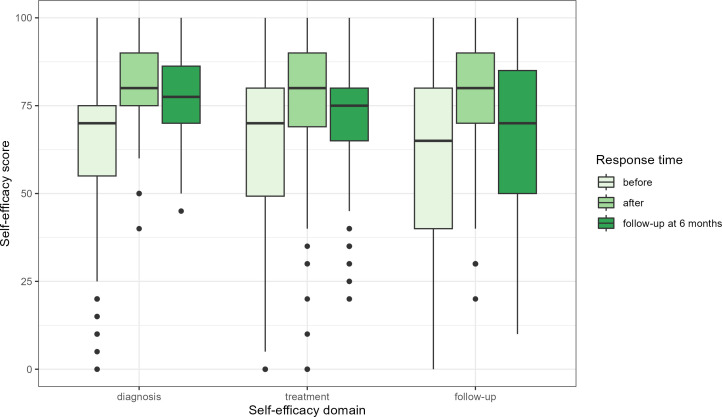
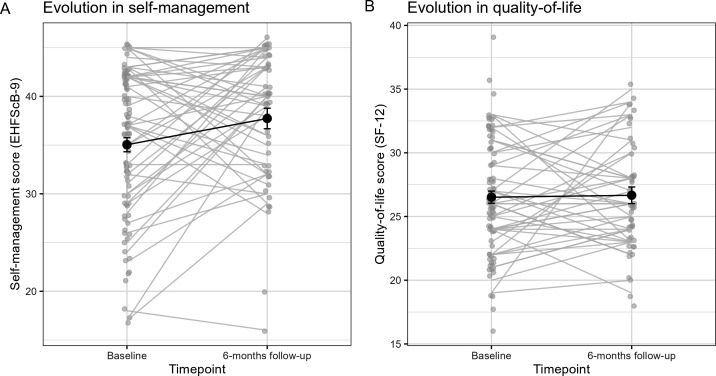
Primary outcomes included GP self-efficacy in HF management, NP testing rates, HF registration in electronic health records and patient self-efficacy (9-item European Heart Failure Self-Care Behaviour Scale (EHFScB-9)). Secondary outcomes included patient quality of life (Short Form-12 questionnaire (SF-12)), hospital readmission rates and provider satisfaction.
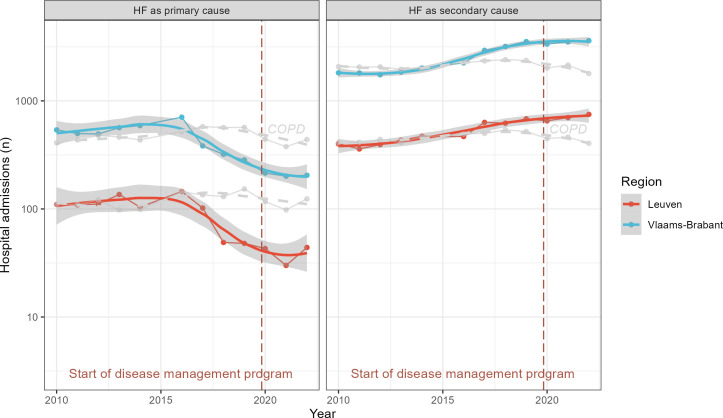
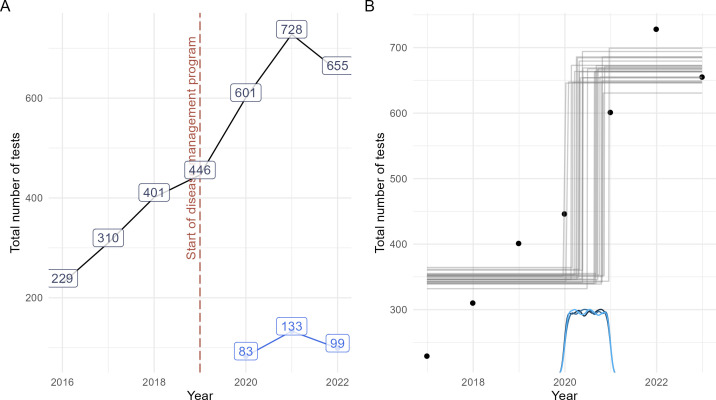
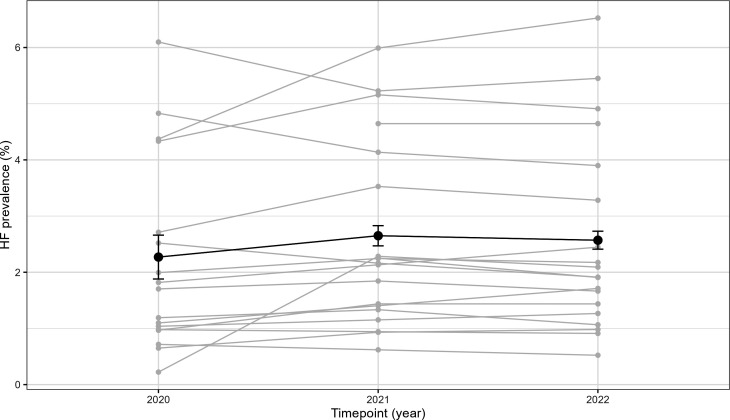
GPs felt more competent in the management of HF after an online education (eight point increase in self-efficacy score after 6 months follow-up, (CI 2.9 to 13, p<0.001)). GPs conducted 314 reimbursed NP tests, half of which scored above age-specific thresholds for referral. After initiation, there was a significant increase in NP testing (Bayes Factor 64), with a total rate of 5.4 tests per 1000 patient years. The proportion of registered HF in patients aged 40 years or older in GPs' electronic health records increased from 2.27% to 2.57% between 2020 and 2022. 96 patients were included in the disease management programme, 75% of these inclusions followed the transitional protocol after discharge for HF. There was significant improvement in patients' self-efficacy after 6-month follow-up (an EHFScB-9 score change of 2.7 points, 95% CI 0.62 to 4.8), but no significant change in quality of life (an SF-12 score change of 0.15 points, 95% CI -1.1 to 1.4). Adherence to the transitional protocol depended on the presence of a specialist HF nurse during admission, 84% of all patients were seen within 14 days after discharge by their general practitioner. Time-trend analysis revealed an increase of HF as a secondary rather than primary cause of admission. Participating healthcare professionals reported satisfaction with the programme.
The IMPACT-B study demonstrated that an integrated disease management programme for HF could be implemented and assessed in routine clinical practice. The programme resulted in increased awareness and registration of HF in primary care, increased self-management of patients and improved follow-up after discharge, although these results should be interpreted cautiously given the uncontrolled pre-post study design.
Trial registration NCT04334447 (clinicaltrials.gov).
心力衰竭是一个重要的健康问题,患者通常年龄较大且伴有多种合并症。因此,推荐进行多学科心力衰竭护理。然而,在现实环境中,关于如何让初级保健卫生专业人员参与以及如何评估此类项目的证据很少。本研究的主要目的是在初级保健环境中整合并评估几种疾病管理干预措施。
前瞻性、非随机、观察性实施研究,采用混合方法进行过程评估,为期3年(2020 - 2022年)。
比利时鲁汶地区的初级保健机构和两家地区医院(一家三级医院,一家二级医院),服务约10万居民。
来自19家医疗机构的100名全科医生(GPs)参与。共有96名患者纳入疾病管理项目。患者的纳入标准包括基于临床标准的心力衰竭(HF)再入院高风险状态。排除标准未明确界定,但参与需要知情同意。
实施了四项干预措施:(1)为全科医生提供在线HF教育;(2)报销利钠肽(NP)检测费用;(3)由经过培训的初级保健HF教育工作者对患者进行教育;(4)出院后结构化的过渡护理方案。
主要结局包括全科医生在HF管理方面的自我效能感、NP检测率、电子健康记录中的HF登记情况以及患者的自我效能感(9项欧洲心力衰竭自我护理行为量表(EHFScB - 9))。次要结局包括患者的生活质量(简短形式 - 12问卷(SF - 12))、医院再入院率和提供者满意度。
在线教育后,全科医生在HF管理方面感觉更有能力(随访6个月后自我效能感得分提高8分,(CI 2.9至13,p < 0.001))。全科医生进行了314次报销的NP检测,其中一半得分高于特定年龄的转诊阈值。启动后,NP检测显著增加(贝叶斯因子64),总检测率为每1000患者年5.4次。2020年至2022年期间,全科医生电子健康记录中40岁及以上患者的HF登记比例从2.27%增加到2.57%。96名患者纳入疾病管理项目,其中75%的纳入患者在出院后遵循了HF过渡方案。随访6个月后患者的自我效能感有显著改善(EHFScB - 9得分变化2.7分,95% CI 0.62至4.8),但生活质量无显著变化(SF - 12得分变化0.15分,95% CI - 1.1至1.4)。对过渡方案的依从性取决于入院时是否有专科HF护士,所有患者中有84%在出院后14天内由其全科医生诊治。时间趋势分析显示,HF作为入院的次要而非主要原因有所增加。参与的医疗保健专业人员对该项目表示满意。
IMPACT - B研究表明,针对HF的综合疾病管理项目可在常规临床实践中实施和评估。该项目导致初级保健中对HF的认识和登记增加,患者的自我管理能力提高,出院后随访改善,尽管鉴于前后对照研究设计未设对照组,这些结果应谨慎解读。
试验注册号NCT04334447(clinicaltrials.gov)。