Wang Ziyi, Guo Jiaojiao, Schaft Eline, Hoogteijling Sem, Ferrier Cyrille H, Visser Gerhard H, Sun Dongqing, Hoefnagels Friso, Inada Taku, van der Salm Sandra, Huiskamp Geertjan, van Klink Nicole, Van't Klooster Maryse, Zijlmans Maeike
Department of Neurology and Neurosurgery, University Medical Center Utrecht Brain Center, University Medical Center Utrecht, Part of ERN EpiCARE, P.O. box 85500, 3508 GA Utrecht, the Netherlands.
Stichting Epilepsie Instellingen Nederland (SEIN), the Netherlands.
Clin Neurophysiol Pract. 2025 Jul 1;10:246-255. doi: 10.1016/j.cnp.2025.06.007. eCollection 2025.
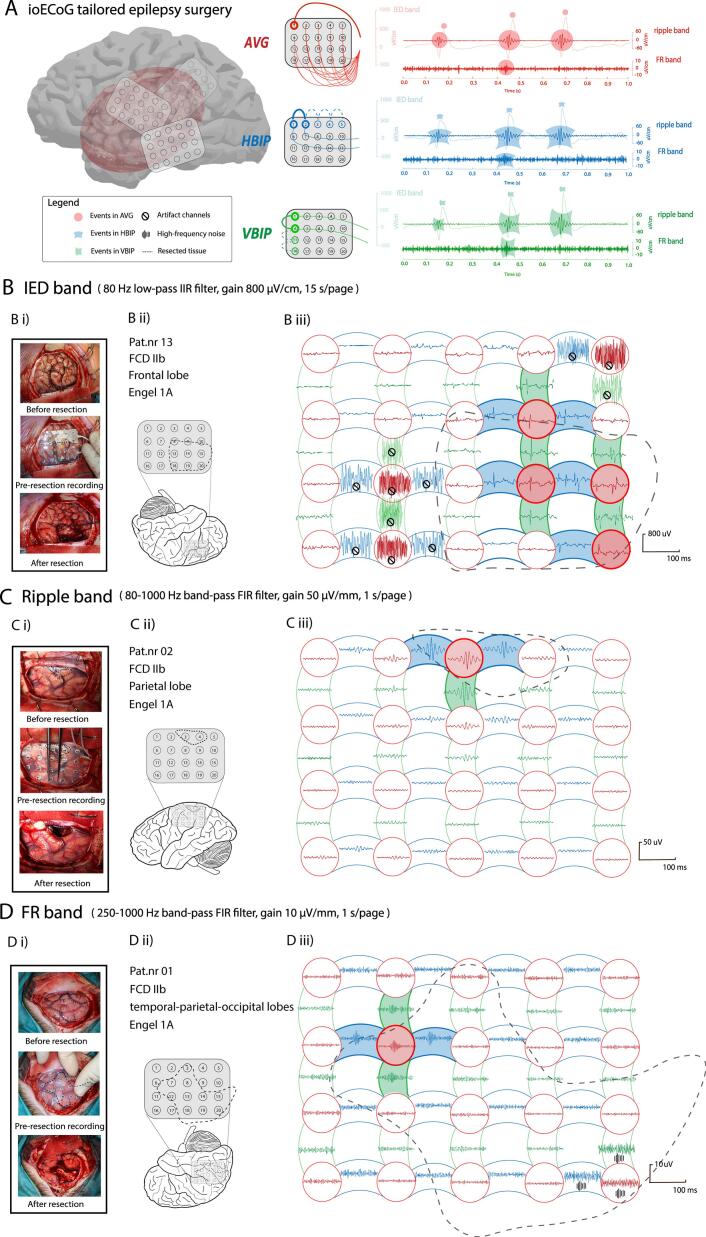
In intraoperative electrocorticography (ioECoG), interictal epileptiform discharges (IEDs) and high-frequency oscillations (HFOs; ripples 80-250 Hz, fast ripples (FRs) 250-500 Hz) can be identified in or montage. We studied how montage choice affects event identification.
Two reviewers independently marked IEDs and HFOs across three montages ( horizontal- and vertical-) from 13 patients who were seizure-free after ioECoG-guided surgery. We analyzed the number of channels-with-events, total events count, events morphology (maximum-amplitude, duration, frequency), number of instances with overlapping events across multiple channels (event_instance), concordance of event_instances over montages, and percentage of channels-with-events in the resected-area.
montages yielded more channels-with-events, higher counts, and greater maximum-amplitude of IEDs and ripples compared to montages. and horizontal montages yielded more IED_instances than vertical montages. montages detected the highest percentage of event_instances occurring only in this montage. Event duration, frequency, and percentage of channels-with-events in the resected-area did not differ across montages.
All three ioECoG montages are clinically useful to find epileptic events. The montage detects more events with greater amplitude, while the montage uncovers a wider variety of unique events. Combining montages provides complementary information.
This study quantitatively revealed how different montages capture epileptiform events.
在术中皮质脑电图(ioECoG)中,可在[具体导联方式1]或[具体导联方式2]导联中识别发作间期癫痫样放电(IEDs)和高频振荡(HFOs;80 - 250Hz的涟漪波,250 - 500Hz的快涟漪波(FRs))。我们研究了导联方式的选择如何影响事件识别。
两名 reviewers 独立标记了来自13例在 ioECoG 引导手术术后无癫痫发作患者的三个导联([水平导联方式]和[垂直导联方式])中的 IEDs 和 HFOs。我们分析了有事件的通道数量、事件总数、事件形态(最大振幅、持续时间、频率)、多个通道上事件重叠的实例数量(事件实例)、不同导联间事件实例的一致性以及切除区域中有事件的通道百分比。
与[另一导联方式]导联相比,[某导联方式]导联产生了更多有事件的通道、更高的计数以及 IEDs 和涟漪波更大幅度。[某导联方式]和水平导联产生的 IED 实例比垂直导联更多。[某导联方式]导联检测到仅在该导联中出现的事件实例的最高百分比。不同导联间事件持续时间、频率以及切除区域中有事件的通道百分比没有差异。
所有三种 ioECoG 导联在临床上都有助于发现癫痫事件。[某导联方式]导联检测到更多振幅更大的事件,而[另一导联方式]导联发现了更广泛的独特事件。联合导联提供了互补信息。
本研究定量揭示了不同导联如何捕捉癫痫样事件。