Burka Semenawit, Aneni Ehimen, Leucker Thorsten, Blaha Michael J
Division of Cardiology, Ciccarone Center for the Prevention of Cardiovascular Disease, Johns Hopkins University School of Medicine, 600 N. Wolfe St., Baltimore, MD 2287, United States.
Section of Cardiovascular Medicine, Department of Internal Medicine, Yale School of Medicine: 175 Sherman Ave, New Haven, CT 06511, United States.
Am J Prev Cardiol. 2025 Jun 26;23:101047. doi: 10.1016/j.ajpc.2025.101047. eCollection 2025 Sep.
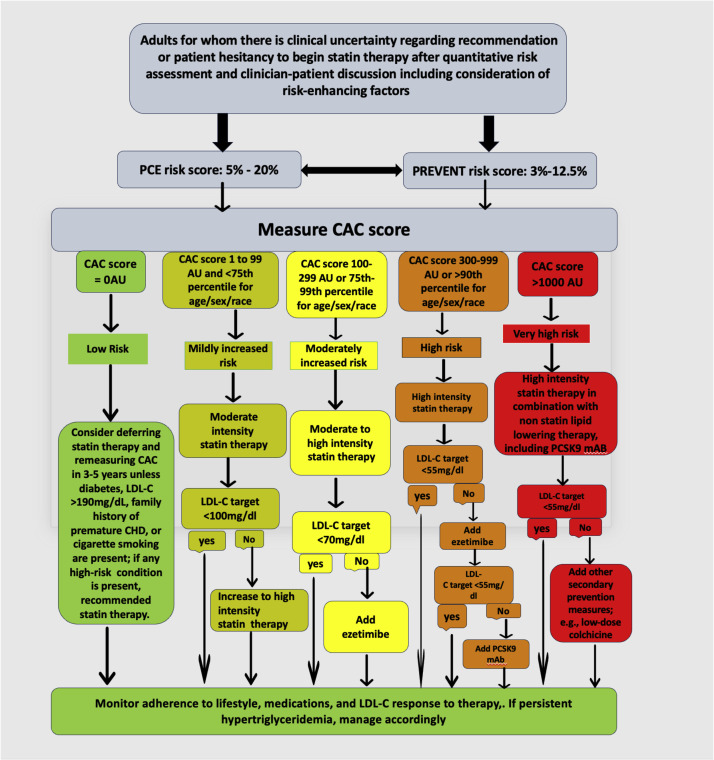
The approach to LDL-C management in primary prevention has shifted from lipid-centric strategies to personalized, risk-based frameworks. However, the binary distinction between primary and secondary prevention may overlook individuals with advanced subclinical atherosclerosis. Coronary artery calcium (CAC) scoring has become central in identifying such patients, especially those whose risk exceeds that implied by traditional risk calculators. The 2022 ACC Expert Consensus Decision Pathway (ECDP) incorporated CAC into LDL-C goal-setting, advocating for LDL-C < 70 mg/dL when CAC >100 or >75th percentile. Emerging evidence suggests that CAC ≥300 portends risk comparable to clinical ASCVD, warranting even lower targets (<55 mg/dL). This editorial highlights how Figure 6 from the 2022 ECDP offers a framework for reclassifying high-risk individuals and recommends that future guidelines recognize CAC >300 as equivalent to secondary prevention.
一级预防中低密度脂蛋白胆固醇(LDL-C)管理方法已从以脂质为中心的策略转向个性化、基于风险的框架。然而,一级预防和二级预防之间的二元区分可能会忽略患有晚期亚临床动脉粥样硬化的个体。冠状动脉钙化(CAC)评分已成为识别此类患者的核心,尤其是那些风险超过传统风险计算器所暗示风险的患者。2022年美国心脏病学会专家共识决策路径(ECDP)将CAC纳入LDL-C目标设定,提倡当CAC>100或>第75百分位数时,LDL-C<70mg/dL。新出现的证据表明,CAC≥300预示的风险与临床动脉粥样硬化性心血管疾病(ASCVD)相当,需要更低的目标(<55mg/dL)。这篇社论强调了2022年ECDP中的图6如何为重新分类高危个体提供了一个框架,并建议未来的指南将CAC>300视为等同于二级预防。