Di Maira Tommaso, Cailliez Valérie, Domínguez-Gil Beatriz, Mahíllo Beatriz, Álvarez Marina, Belli Luca Saverio, Adam René, Fondevila Constantino, Germani Giacomo, Hartog Hermien, Berenguer Marina
Liver Transplantation and Hepatology Unit, Hospital Universitari I Politècnic La Fe, Valencia, Spain.
CIBERehd, Instituto de Salud Carlos III, Madrid, Spain, IIS La Fe, Valencia, Spain.
JHEP Rep. 2025 Apr 11;7(8):101424. doi: 10.1016/j.jhepr.2025.101424. eCollection 2025 Aug.
BACKGROUND & AIMS: Liver transplantation (LT) is a live-saving therapy for patients with end-stage liver disease, but demand exceeds supply, leading to waiting list (WL) mortality. This study reviews LT practices and trends in Europe to identify potential policies for improving outcomes.
Data were extracted from the European Liver Transplant Registry and the Global Observatory on Donation and Transplantation. Countries were categorized into Eastern (EEC), Mediterranean (MEC), and Northern European (NEC). We analyzed LT indications, recipient and donor age, transplant type, and WL outcomes from 2012 to 2022.
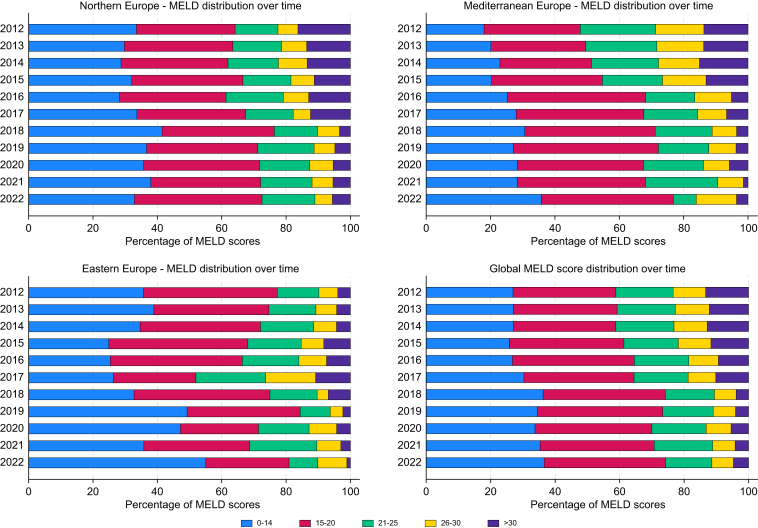
Etiology of LT differed across regions: HBV cirrhosis predominated in EEC (37.3%), whereas alcohol-related liver disease was more frequent in NEC (41.8%) and MEC (49.1%). Metabolic-dysfunction associated steatotic liver disease increased across Europe, particularly in NEC. Recipient age has risen, with 40% aged ≥60 years in MEC 20% in EEC. Donor age and type also varied: EEC relies on younger donors (<50 years, 70%), whereas MEC expanded criteria to include donors ≥60 years (50%). Donation after circulatory determination of death increased by 30%, particularly in NEC and MEC, but remains rare in EEC. Model for end-stage liver disease scores at LT decreased, with 30% scoring >21 in 2021 50% in 2012. WL mortality declined by 10% since 2015, although large inter-country variability persists.
LT practices in Europe are highly heterogeneous. Regional disparities in recipient profiles, donor characteristics, and transplant modalities reflect varying policies and healthcare capacities. Expanding donor criteria and harmonizing allocation systems are required to reduce WL mortality and improve access to LT across Europe.
This study provides a comprehensive analysis of liver transplantation practices across Europe, highlighting significant regional disparities in donor criteria, allocation systems, and transplant outcomes. By identifying trends such as the expansion of Donation after Circulatory Determination of Death programs and the prioritization of model for end-stage liver disease ≥30 policies, these findings underscore the critical need for harmonized strategies to reduce waiting list mortality and improve access to transplantation. The results are particularly relevant for policymakers and healthcare administrators seeking to optimize liver transplant systems, and for clinicians aiming to adopt best practices from high-performing regions. Practical applications include refining allocation policies, expanding donor pools, and addressing regional inequalities, all while considering the limitations posed by diverse healthcare infrastructures and socioeconomic factors.
肝移植(LT)是终末期肝病患者的一种挽救生命的治疗方法,但需求超过供给,导致等待名单(WL)死亡率上升。本研究回顾了欧洲的肝移植实践和趋势,以确定改善治疗结果的潜在政策。
数据从欧洲肝移植登记处和全球捐赠与移植观察站提取。国家被分为东欧(EEC)、地中海地区(MEC)和北欧(NEC)。我们分析了2012年至2022年期间的肝移植适应症、受者和供者年龄、移植类型以及等待名单结果。
不同地区肝移植的病因有所不同:EEC地区以乙肝肝硬化为主(37.3%),而NEC地区(41.8%)和MEC地区(49.1%)与酒精相关的肝病更为常见。代谢功能障碍相关脂肪性肝病在欧洲各地都有所增加,尤其是在NEC地区。受者年龄有所上升,MEC地区40%的受者年龄≥60岁,EEC地区为20%。供者年龄和类型也各不相同:EEC地区依赖较年轻的供者(<50岁,70%),而MEC地区扩大了标准,将≥60岁的供者纳入其中(50%)。循环判定死亡后捐赠增加了30%,尤其是在NEC地区和MEC地区,但在EEC地区仍然很少见。肝移植时终末期肝病模型评分有所下降,2021年评分>21的患者为30%,2012年为50%。自2015年以来,等待名单死亡率下降了10%,尽管国家间仍存在较大差异。
欧洲的肝移植实践高度异质。受者特征、供者特点和移植方式的地区差异反映了不同的政策和医疗保健能力。需要扩大供者标准并统一分配系统,以降低等待名单死亡率并改善欧洲各地肝移植的可及性。
本研究对欧洲各地的肝移植实践进行了全面分析,突出了供者标准、分配系统和移植结果方面显著的地区差异。通过识别循环判定死亡后捐赠项目扩大和终末期肝病模型≥30政策优先等趋势,这些发现强调了采取统一策略以降低等待名单死亡率和改善移植可及性的迫切需求。这些结果对于寻求优化肝移植系统的政策制定者和医疗保健管理人员,以及旨在采用高绩效地区最佳实践的临床医生尤为相关。实际应用包括完善分配政策、扩大供者库和解决地区不平等问题,同时考虑到不同医疗基础设施和社会经济因素带来的限制。