Rakotozandrindrainy Njariharinjakamampionona, Kang Sophie S Y, Wandji Nana Lady R, Sugimoto Jonathan D, Wang Yi-Ting, Rakotozandrindrainy Ndrainaharimira, Razafindrabe Tsiriniaina Jean Luco, Raminosoa Tiana Mirana, Hong Sye Lim, Razafindrakalia Mathilde, Nyirenda Gabriel, Binger Tabea, Higginson Ellen E, Jeon Hyon Jin, Wangmo Namgay, Cakpo Gbènonminvo E, You YoungAe, Tadesse Birkneh Tilahun, Soura Abdramane Bassiahi, Rakotozandrindrainy Raphaël, Marks Florian
Madagascar Institute for Vaccine Research, University of Antananarivo, Antananarivo, Madagascar.
International Vaccine Institute, SNU Research Park, Seoul, Korea, Republic of Korea.
Clin Infect Dis. 2025 Jul 22;80(Supplement_1):S16-S28. doi: 10.1093/cid/ciaf041.
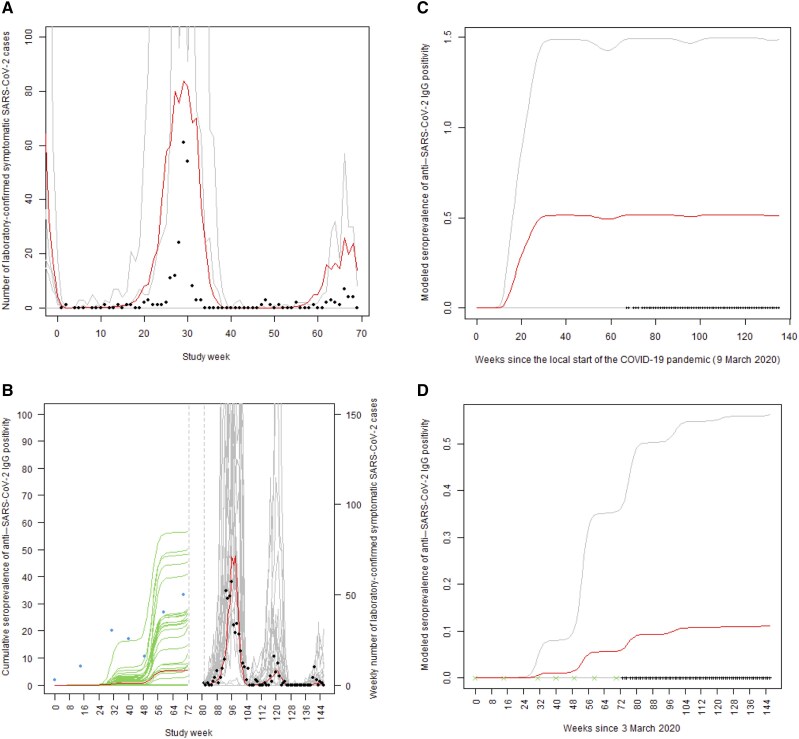
Coronavirus disease 2019 (COVID-19) caused substantial disease and death worldwide since December 2019, but the burden was lower in Africa than in high-income countries. To address potential underreporting, we modeled severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and disease burden in Burkina Faso and Madagascar.
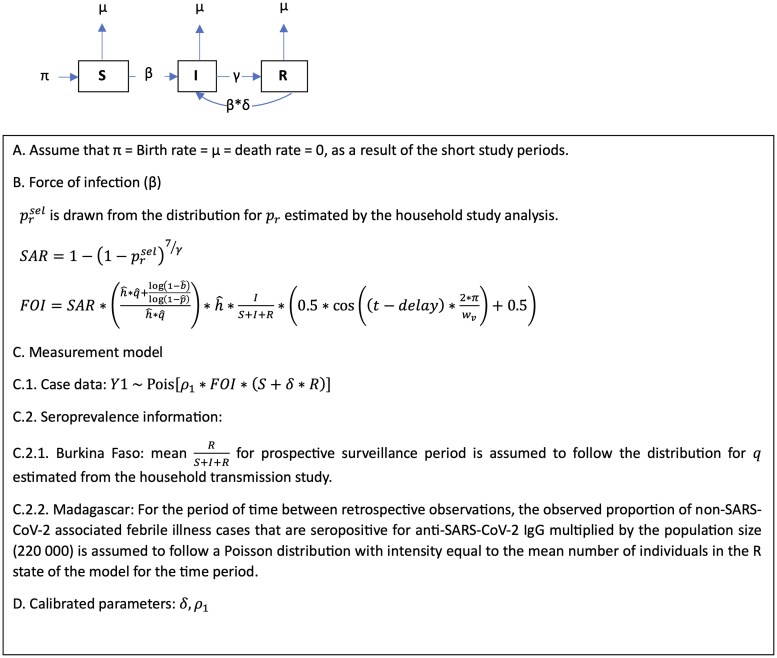
Prospectively enrolled patients who presented with fever at sentinel healthcare facilities were assessed for active SARS-CoV-2 infection. Household members of SARS-CoV-2-infected patients were prospectively followed for confirmed SARS-CoV-2 infection. Archived serum specimens that spanned the pandemic onset in Madagascar to the start of prospective surveillance were tested for anti-SARS-CoV-2 immunoglobulins. Data from these multiple sources contributed to an integrated analysis to calibrate an epidemiologic mass action model.
COVID-19 accounted for a substantial fraction of healthcare-ascertained febrile illness in both Burkina Faso and Madagascar, with symptom profiles consistent with those previously reported. SARS-CoV-2 vaccination coverage was very low in Burkina Faso and unavailable in Madagascar. The household secondary attack rate was 28% (95% confidence intervals [CI], 22%-35%] in Madagascar and 31% (95% CI: 9%-68%) in Burkina Faso, indicating substantial transmission of the disease within households in both locations. Model simulations estimated that the actual number of SARS-CoV-2 infections was at least nine times higher than the reported number of febrile COVID-19 cases.
Africa has faced persistent challenges due to underinvestment in vaccination programs and disease surveillance programs. There was substantial underreporting of COVID-19 cases during the pandemic in both countries. Our findings call for improving systems and resources in disease surveillance during epidemic and interepidemic periods in these countries.
自2019年12月以来,2019冠状病毒病(COVID-19)在全球范围内造成了大量疾病和死亡,但非洲的负担低于高收入国家。为了解决潜在的报告不足问题,我们对布基纳法索和马达加斯加的严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染及疾病负担进行了建模。
对在前瞻性哨点医疗机构出现发热症状的患者进行主动评估,以确定是否存在活动性SARS-CoV-2感染。对SARS-CoV-2感染患者的家庭成员进行前瞻性随访,以确认是否感染SARS-CoV-2。对马达加斯加疫情开始至前瞻性监测开始期间存档的血清标本进行抗SARS-CoV-2免疫球蛋白检测。这些多源数据有助于进行综合分析,以校准一个流行病学群体作用模型。
在布基纳法索和马达加斯加,COVID-19在通过医疗保健确诊的发热性疾病中占很大比例,症状特征与先前报告的一致。布基纳法索的SARS-CoV-2疫苗接种覆盖率非常低,马达加斯加则无法获得疫苗。马达加斯加的家庭二代发病率为28%(95%置信区间[CI],22%-35%),布基纳法索为31%(95%CI:9%-68%),表明两地家庭内该疾病均有大量传播。模型模拟估计,SARS-CoV-2实际感染人数至少比报告的发热COVID-19病例数高九倍。
由于疫苗接种计划和疾病监测计划投资不足,非洲一直面临持续挑战。在这两个国家的疫情期间,COVID-19病例存在大量漏报情况。我们的研究结果呼吁在这些国家的流行期间和流行间期改善疾病监测系统和资源。