Groenland Carline N L, Janssen Matthijs L, van den Bosch Kim S, Baggen Vivan J M, Heunks Leo, Endeman Henrik, Wils Evert-Jan
Intensive Care, Franciscus Gasthuis en Vlietland, Rotterdam, The Netherlands.
Intensive Care, Erasmus MC, Rotterdam, The Netherlands.
BMJ Open Respir Res. 2025 Jul 21;12(1):e002868. doi: 10.1136/bmjresp-2024-002868.
Liberation from invasive mechanical ventilation is a milestone in critical care, but approaches vary. This survey aimed to describe current ventilator liberation practices, relate them to available evidence, and identify areas for improvement.
A survey was performed among Dutch intensive care unit (ICU) sites. The survey evaluated practice in seven domains of ventilator liberation: protocol availability, transition from controlled to assisted ventilation, spontaneous breathing trials (SBT), cuff-leak test, postextubation support, weaning failure and tracheostomised weaning.
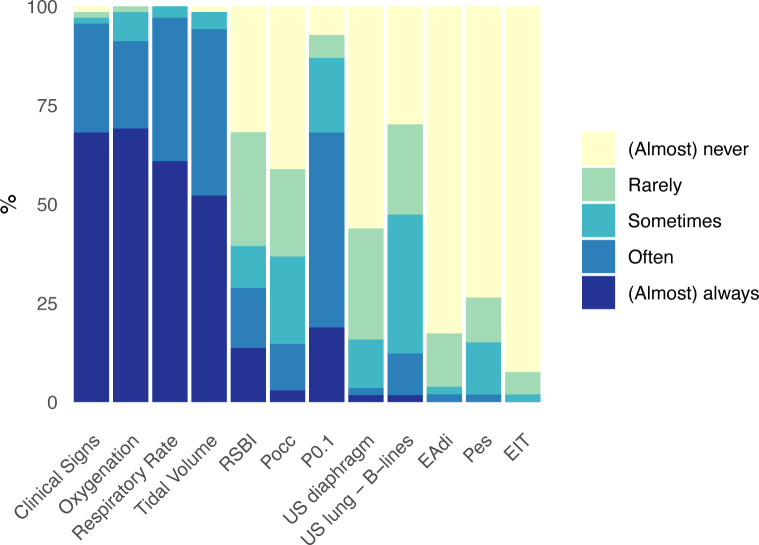
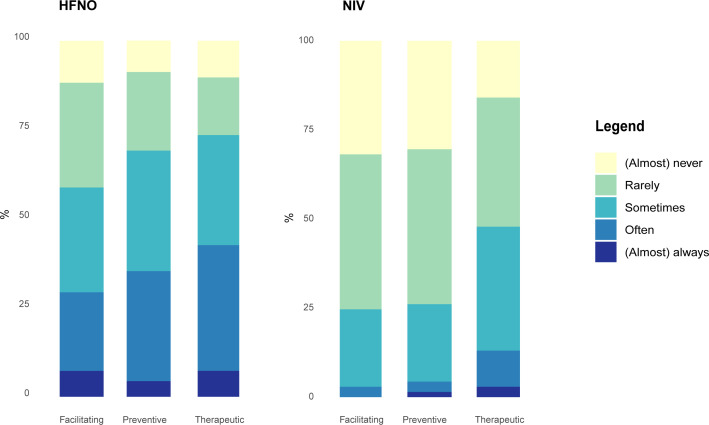
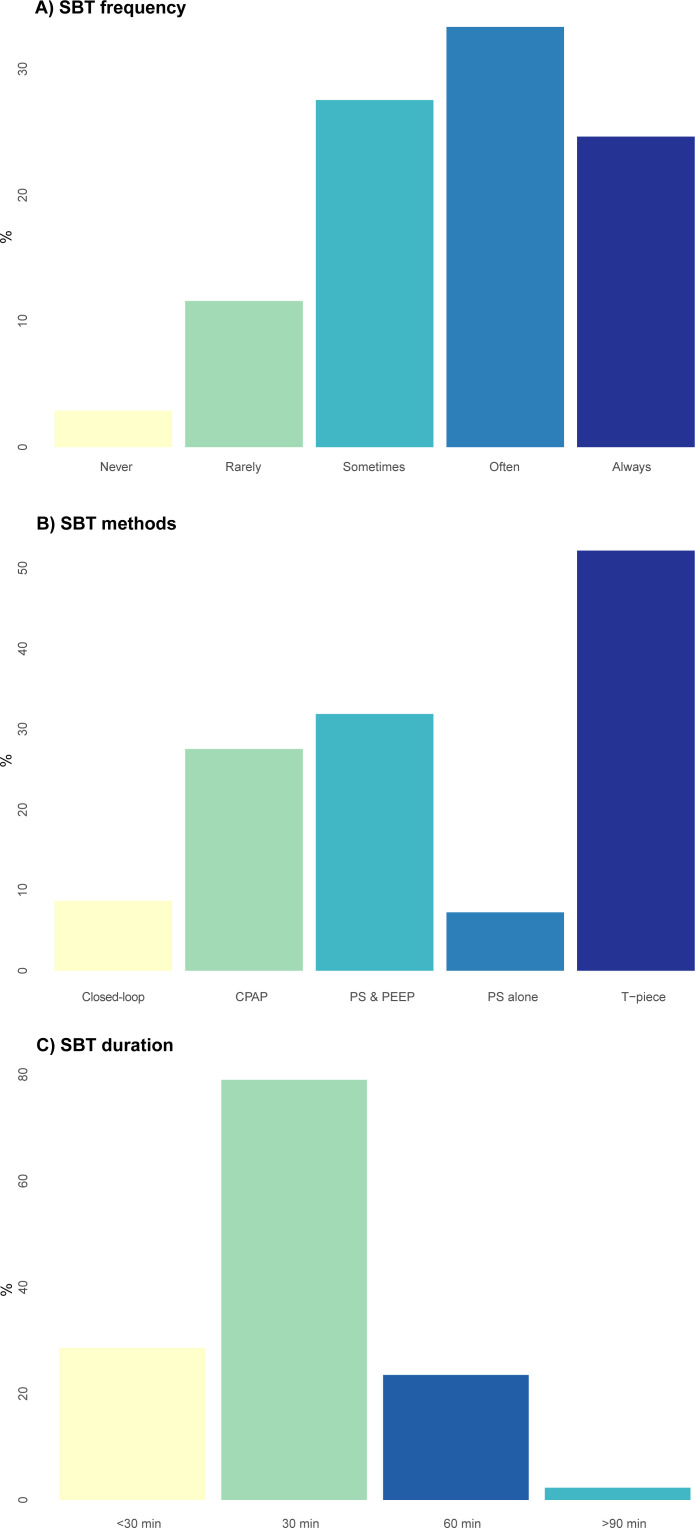
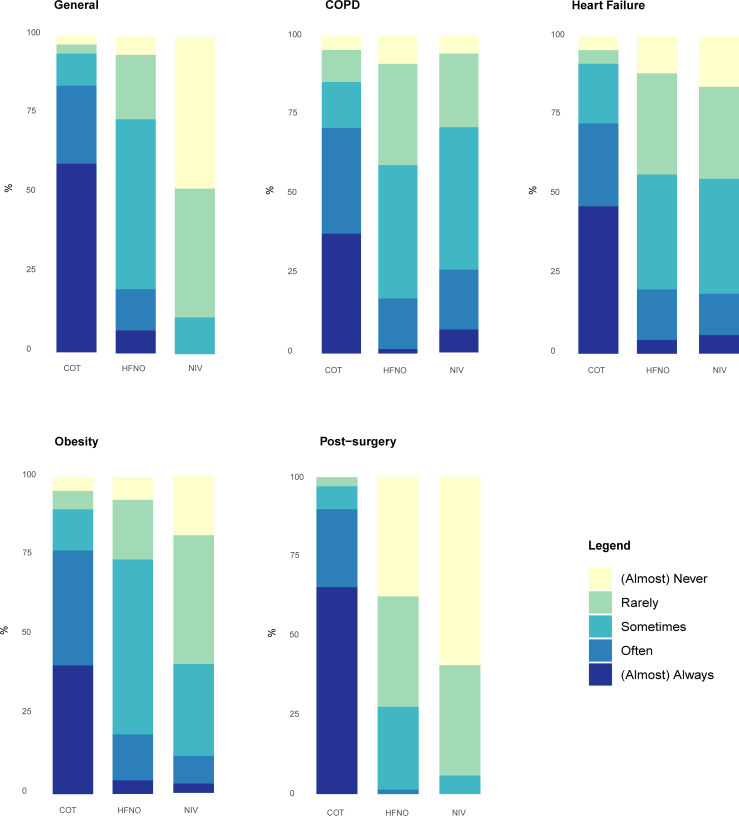
The survey response rate was 93% (132/142), representing 97% (69/71) of Dutch ICUs. Protocols for postextubation support and weaning failure were available in less than half of the ICUs (44% and 49%, respectively). The transition from controlled to assisted ventilation is regularly evaluated daily in 78% of ICUs. Assisted ventilation tolerance is mainly assessed by clinical signs, respiratory parameters and non-invasive manoeuvres that assess respiratory drive (P). SBTs are regularly performed in 58% of ICUs, using one or more of the following methods: T-piece (52%), pressure support+positive end expiratory pressure (32%) and continuous positive airway pressure (28%). Cuff-leak tests are seldom performed (1.4%), predominantly in cases of intubation for upper-airway obstruction (92%). Postextubation respiratory support with high-flow nasal oxygen or non-invasive ventilation is used at least as often with therapeutic (43%/13%) rather than preventive (35%/4%) of facilitative intent (29%/3%). Delirium screening (87%) and reconsidering sedation (84%) are frequently assessed in case of weaning failure. Regular use of closed-loop ventilation is reported in a minority of ICUs throughout the process of ventilator liberation (3-9%).
Various aspects of ventilator liberation practices show only limited alignment with existing guidelines. The results of this survey pinpoint areas to prioritise in guideline and practice improvement.
从有创机械通气中撤机是重症监护中的一个里程碑,但方法各不相同。本调查旨在描述当前的呼吸机撤机实践,将其与现有证据相关联,并确定改进领域。
对荷兰重症监护病房(ICU)进行了一项调查。该调查评估了呼吸机撤机七个领域的实践情况:方案可用性、从控制通气到辅助通气的转换、自主呼吸试验(SBT)、套囊漏气试验、拔管后支持、撤机失败和气管切开患者的撤机。
调查回复率为93%(132/142),占荷兰ICU的97%(69/71)。不到一半的ICU有拔管后支持和撤机失败的方案(分别为44%和49%)。78%的ICU每天定期评估从控制通气到辅助通气的转换。辅助通气耐受性主要通过临床体征、呼吸参数和评估呼吸驱动的非侵入性操作(P)来评估。58%的ICU定期进行SBT,使用以下一种或多种方法:T形管(52%)、压力支持+呼气末正压(32%)和持续气道正压(28%)。很少进行套囊漏气试验(1.4%),主要用于上气道梗阻插管病例(92%)。拔管后使用高流量鼻氧或无创通气进行呼吸支持时,至少同样常用于治疗目的(43%/13%)而非预防目的(35%/4%)或促进目的(29%/3%)。在撤机失败时,经常评估谵妄筛查(87%)和重新考虑镇静(84%)。在呼吸机撤机的整个过程中,少数ICU报告经常使用闭环通气(3-9%)。
呼吸机撤机实践的各个方面与现有指南的一致性有限。本次调查结果指出了在指南和实践改进中应优先考虑的领域。