Fehlings Michael G, Pedro Karlo M, Alvi Mohammed Ali, Moghaddamjou Ali, Harrop James S, Stanford Ralph, Ball Jonathon, Aarabi Bizhan, Arnold Paul M, Guest James D, Kurpad Shekar N, Schuster James M, Nassr Ahmad N, Schmitt Karl M, Wilson Jefferson R, Brodke Darrel S, Ahmad Faiz U, Yee Albert, Ray Wilson Z, Brooks Nathaniel P, Wilson Jason, Chow Diana S-L, Toups Elizabeth G, Thorpe Kevin E, Huang Jiaxin, Huang Peng
Division of Neurosurgery and Spine Program, Department of Surgery, University of Toronto, Toronto, ON, Canada; Division of Neurosurgery, Krembil Neuroscience Centre, Toronto Western Hospital, University Health Network, Toronto, ON, Canada; Institute of Medical Science, University of Toronto, Toronto, ON, Canada.
Division of Neurosurgery and Spine Program, Department of Surgery, University of Toronto, Toronto, ON, Canada; Division of Neurosurgery, Krembil Neuroscience Centre, Toronto Western Hospital, University Health Network, Toronto, ON, Canada; Institute of Medical Science, University of Toronto, Toronto, ON, Canada.
EBioMedicine. 2025 Jul 24;118:105863. doi: 10.1016/j.ebiom.2025.105863.
Spinal cord injury (SCI) clinical trials typically rely on a single primary endpoint to assess drug efficacy. This strategy fails to adequately capture the full impact of treatment in heterogenous neurological conditions like SCI. A more patient-centric analysis requires assessment of neurological function, functional capacity, and quality of life, incorporating meaningful patient-reported outcomes. The global statistical test (GST) addresses this challenge using a unified statistical conclusion regarding the superiority of a treatment strategy over another by evaluating multiple trial endpoints simultaneously.
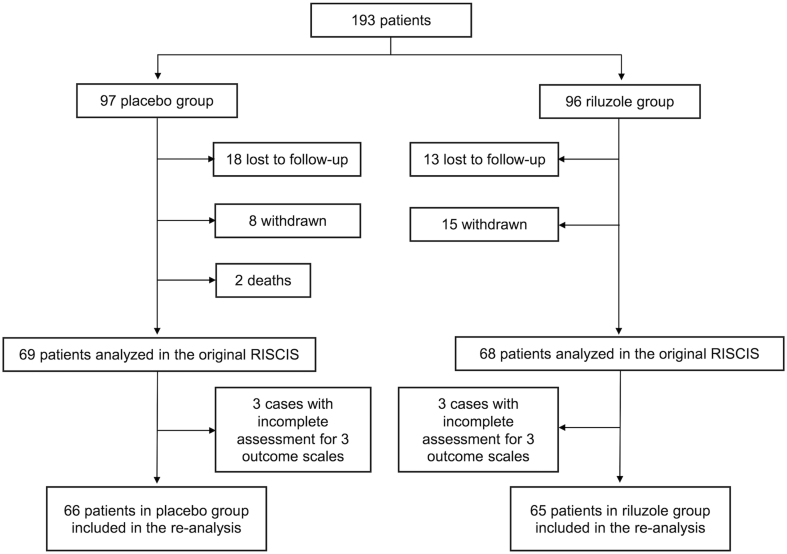
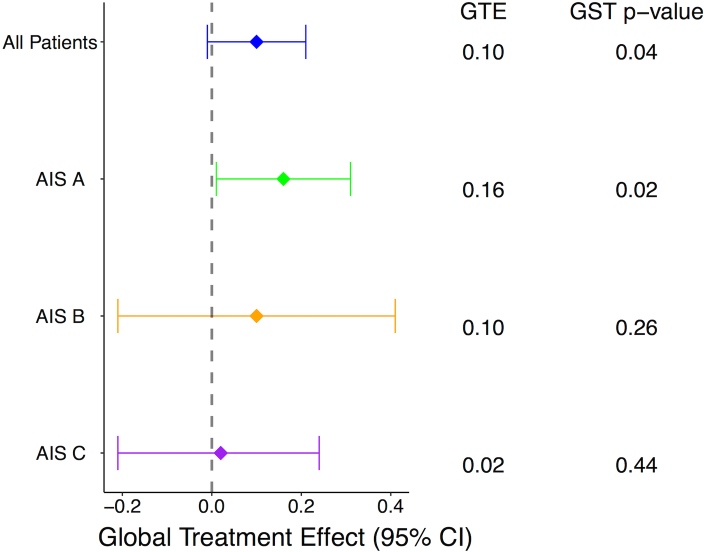
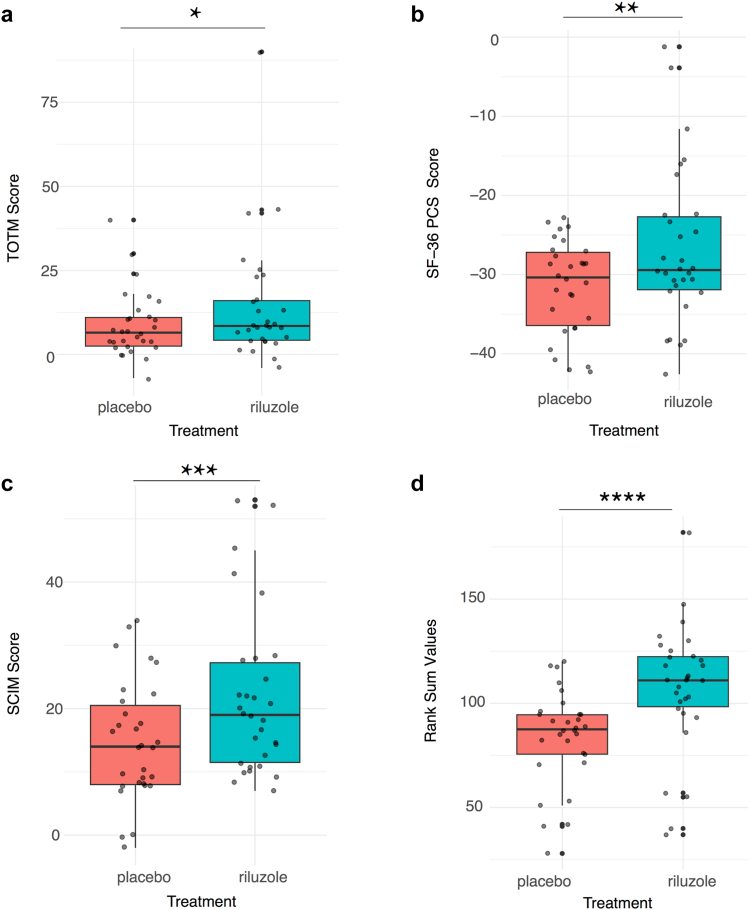
The RISCIS trial (Safety and Efficacy of Riluzole in Acute Spinal Cord Injury Study) data was analysed using a multivariate nonparametric GST, integrating the total American Spinal Injury Association (ASIA) motor score (TOTM), Spinal Cord Independence Measure (SCIM), and SF-36 PCS (Short Form-36 Physical Component Scale) scores. In the RISCIS trial, patients with severe cervical SCI (AIS A, B, and C) were randomised to receive riluzole or placebo within 12 h of injury in a double blinded fashion. We compared six-month outcomes between groups using a modified O'Brien's rank sum test with sample variance adjustment. Higher summed ranks represent better global outcomes. The overall probability of improvement was computed using a summary estimate, the global treatment effect (GTE).
A total of 131 patients (mean age 45.8 years old, 82% males) completed the six-month outcome assessment. Among these, 49.6% were classified as AIS A, 20.6% as AIS B, and 29% as AIS C. Riluzole was administered within 12 h from injury for 14 days in 65 patients, while 66 received a placebo. The unadjusted mean change from baseline to six months showed a favourable response in the riluzole group compared to placebo across TOTM (p = 0.28 by t-test; p = 0.26 by Wilcoxon test), SCIM (p = 0.04 by t-test; p = 0.02 by Wilcoxon test), or SF-36 PCS (p = 0.23 by t-test; p = 0.21 by Wilcoxon test) scores. Using the GST to simultaneously assess these measures, the riluzole group exhibited a higher rank sum compared to placebo [median rank sum = 207 (IQR: 166-246) in riluzole vs 185 (IQR: 146-236) in placebo, p = 0.04]. Subgroup analysis revealed the greatest treatment benefit among patients with AIS A injuries (GTE = 0.16, 95% CI: 0.01-0.31, p = 0.02). At six months, the probability that riluzole treatment resulted in overall better outcomes than placebo across all assessed outcomes was 58%.
Riluzole was associated with improved global outcomes in patients with severe traumatic SCI, based on a composite score integrating ASIA total motor scores, SCIM, and SF36 outcomes at six months. Riluzole is a promising therapeutic option in SCI, but further investigation through higher-quality studies incorporating multidimensional assessments is warranted.
No funding was received for the present work. The original clinical trial (NCT01597518) was funded by the AO Foundation, United States Department of Defense (DOD), and the Praxis Spinal Cord Institute.
脊髓损伤(SCI)临床试验通常依赖单一主要终点来评估药物疗效。这种策略未能充分体现治疗对SCI这类异质性神经疾病的全面影响。更以患者为中心的分析需要评估神经功能、功能能力和生活质量,并纳入有意义的患者报告结局。全局统计检验(GST)通过同时评估多个试验终点,就一种治疗策略相对于另一种治疗策略的优越性得出统一的统计结论,从而应对这一挑战。
使用多变量非参数GST对RISCIS试验(利鲁唑治疗急性脊髓损伤的安全性和有效性研究)数据进行分析,综合美国脊髓损伤协会(ASIA)总运动评分(TOTM)、脊髓独立测量量表(SCIM)和SF-36生理健康分量表(PCS)评分。在RISCIS试验中,重度颈髓SCI(AIS A、B和C级)患者在受伤后12小时内被随机双盲分配接受利鲁唑或安慰剂治疗。我们使用经样本方差调整的改良奥布赖恩秩和检验比较两组的六个月结局。秩和越高代表整体结局越好。使用汇总估计值全局治疗效应(GTE)计算改善的总体概率。
共有131名患者(平均年龄45.8岁,82%为男性)完成了六个月结局评估。其中,49.6%为AIS A级,20.6%为AIS B级,29%为AIS C级。65名患者在受伤后12小时内接受利鲁唑治疗14天,66名患者接受安慰剂治疗。从基线到六个月的未调整平均变化显示,在TOTM(t检验p = 0.28;威尔科克森检验p = 0.26)、SCIM(t检验p = 0.04;威尔科克森检验p = 0.02)或SF-36 PCS(t检验p = 0.23;威尔科克森检验p = 0.21)评分方面,利鲁唑组与安慰剂组相比有良好反应。使用GST同时评估这些指标时,利鲁唑组的秩和高于安慰剂组[利鲁唑组中位数秩和 = 207(IQR:166 - 246),安慰剂组为185(IQR:146 - 236),p = 0.04]。亚组分析显示,AIS A级损伤患者的治疗获益最大(GTE = 0.16,95%CI:0.01 - 0.31,p = 0.02)。六个月时,在所有评估结局方面,利鲁唑治疗总体结局优于安慰剂的概率为58%。
基于综合六个月时的ASIA总运动评分、SCIM和SF36结局的复合评分,利鲁唑与重度创伤性SCI患者的整体结局改善相关。利鲁唑是SCI中有前景的治疗选择,但有必要通过纳入多维评估的高质量研究进一步探究。
本研究未获得资金支持。原临床试验(NCT01597518)由AO基金会、美国国防部(DOD)和普拉西斯脊髓研究所资助。