Kepha Stella, Omondi Wyckliff, Odiere Maurice R, Juma Chitiavi, Muchangi Martin, Wanja Dollycate N, Kanyi Chrisistosom, Oloo Joseph, Ower Alison, Chami Irene Natalie, Matendechero Sultani Hadley, Wakesho Florence
Eastern and Southern Africa Centre of International Parasite Control, Kenya Medical Research Institute, Nairobi, Kenya.
Division of Vector Borne and Neglected Tropical Diseases, Ministry of Health, Nairobi, Kenya.
PLoS Negl Trop Dis. 2025 Jul 28;19(7):e0013233. doi: 10.1371/journal.pntd.0013233. eCollection 2025 Jul.
Mapping of schistosomiasis (SCH) and soil-transmitted helminthiasis (STH) is a critical step in understanding where at-risk populations live in order to effectively plan and target available resources and to achieve maximum impact on disease burden. A precision mapping protocol was developed and implemented in Kakamega, Bungoma, Trans Nzoia and Vihiga Counties in western Kenya by applying the current World Health Organization (WHO) mapping guideline at a lower administrative level (Ward).
Cross-sectional surveys were conducted among school-age children (SAC) in 5 primary schools purposefully selected in each mapping unit (Ward). In each school, stool and urine samples were collected from 60 randomly selected children (ages 8-14 years). The prevalence and intensity of infection of Schistosoma mansoni and STH were determined using the Kato-Katz technique and urine filtration for S. haematobium. Water Sanitation and Hygiene (WASH) status were also recorded.
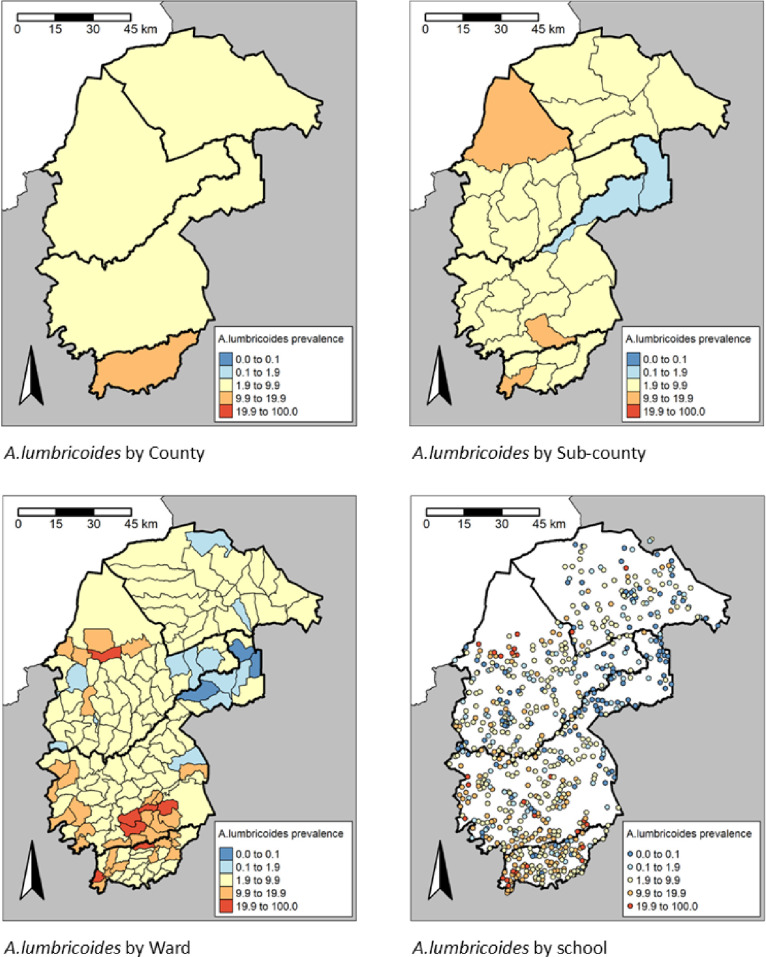
Of the 46,464 children sampled, 3.2% (95% CI: 3.0-3.3) were infected with at least one Schistosoma species, with S. mansoni being the most predominant at 3.2% (95% CI: 2.9 - 3.3). 7.6% (95% CI: 7.3 - 7.8) of children were infected with at least one STH species, with A. lumbricoides being the most common (6.5%), and hookworm the least common (0.7%). The prevalence of S. mansoni was highest in Bungoma County (4.5%) and lowest in Trans Nzoia county (0.5%); STH prevalence was highest in Vihiga County (10.7%) and lowest in Trans Nzoia County (4.8%). SCH and STH infections were mainly of light intensity (2.2% and 5.6%, respectively). Based on sub-County-level data and prevalence threshold of ≥2% for MDA, 49 and 144 Wards required treatment for SCH and STH, respectively, whereas based on the Ward-level data, only 40 and 138 Wards required treatment for SCH and STH, respectively.
Use of Ward relative to sub-county prevalence revealed considerable spatial heterogeneity for SCH and STH and resulted in 14.5% and 0.8% reduction in the number of people treated for SCH and STH, respectively, underscoring the critical role of precision mapping in improved targeting of interventions.
绘制血吸虫病(SCH)和土壤传播的蠕虫病(STH)分布图是了解高危人群居住地点的关键一步,以便有效地规划和分配现有资源,并最大限度地减轻疾病负担。通过在肯尼亚西部的卡卡梅加、邦戈马、特兰斯佐亚和维希加县较低行政级别(选区)应用世界卫生组织(WHO)当前的绘图指南,制定并实施了精确绘图方案。
在每个绘图单元(选区)有目的地选择的5所小学中,对学龄儿童(SAC)进行横断面调查。在每所学校,从60名随机选择的儿童(8 - 14岁)中采集粪便和尿液样本。使用加藤-卡茨技术和尿液过滤法检测曼氏血吸虫和土壤传播的蠕虫病感染率及感染强度,以检测埃及血吸虫。还记录了水、环境卫生和个人卫生(WASH)状况。
在46464名抽样儿童中,3.2%(95%CI:3.0 - 3.3)感染了至少一种血吸虫,其中曼氏血吸虫最为常见,感染率为3.2%(95%CI:2.9 - 3.3)。7.6%(95%CI:7.3 - 7.8)的儿童感染了至少一种土壤传播的蠕虫,其中蛔虫最为常见(6.5%),钩虫最不常见(0.7%)。曼氏血吸虫感染率在邦戈马县最高(4.5%),在特兰斯佐亚县最低(0.5%);土壤传播的蠕虫病感染率在维希加县最高(10.7%),在特兰斯佐亚县最低(4.8%)。血吸虫病和土壤传播的蠕虫病感染主要为轻度感染(分别为2.2%和5.6%)。根据县级以下数据和大规模药物驱虫(MDA)≥2%的流行阈值,分别有49个和144个选区需要进行血吸虫病和土壤传播的蠕虫病治疗,而根据选区级数据,分别只有40个和138个选区需要进行血吸虫病和土壤传播的蠕虫病治疗。
与县级以下流行率相比,使用选区流行率显示出血吸虫病和土壤传播的蠕虫病存在显著的空间异质性,分别使接受血吸虫病和土壤传播的蠕虫病治疗的人数减少了14.5%和0.8%,强调了精确绘图在改进干预措施目标定位方面的关键作用。