Malik Ali, Ippolito Paul, Kundur Sukruth Pradeep, Sivalokanathan Sanjay
Faculty of Life Sciences and Medicine, King's College London, London WC2R SLS, UK.
Department of Cardiology, Icahn School of Medicine at Mount Sinai Morningside, New York, NY 10025, USA.
Reports (MDPI). 2025 Mar 6;8(1):28. doi: 10.3390/reports8010028.
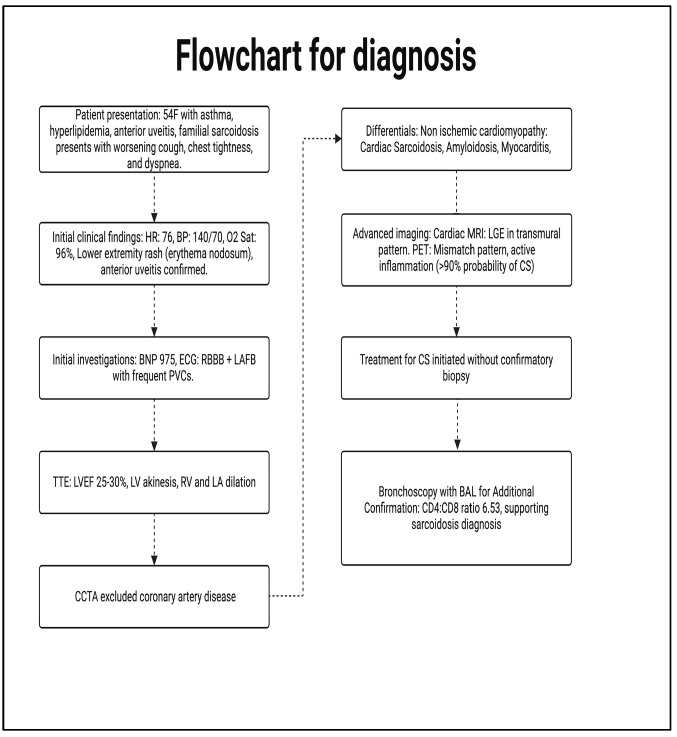
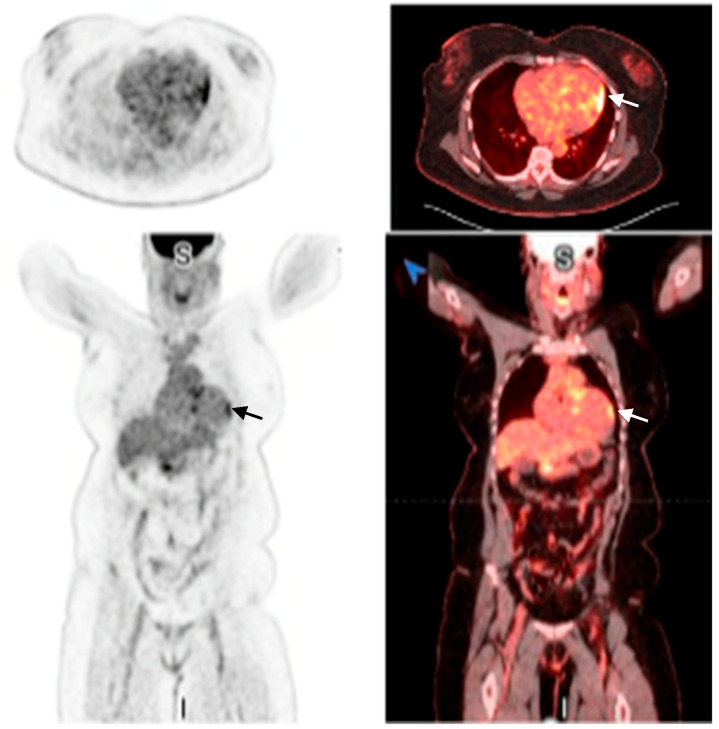
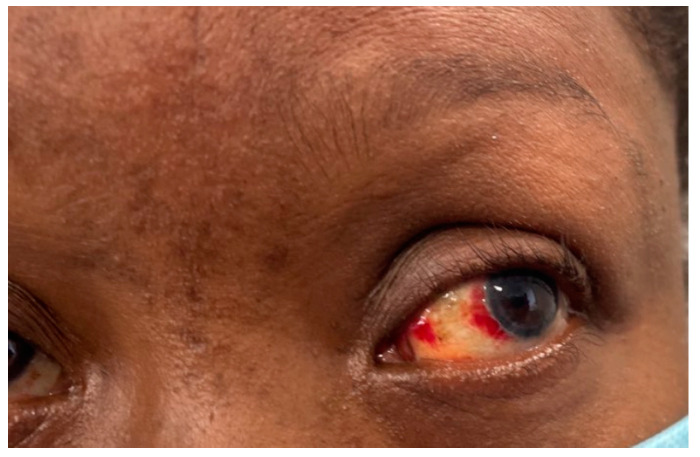
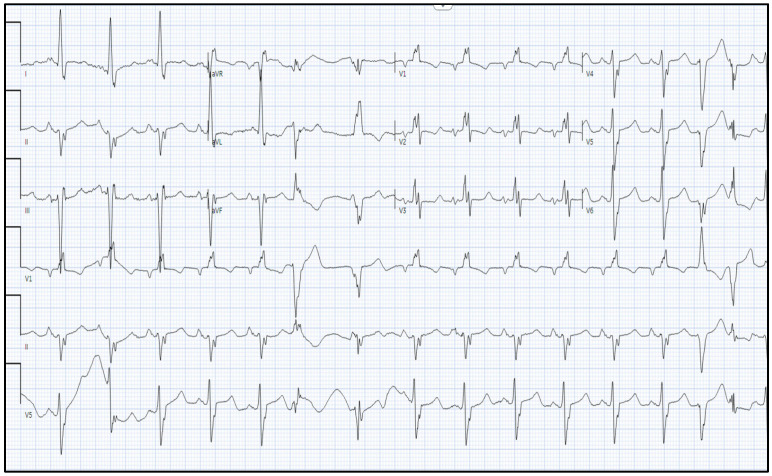
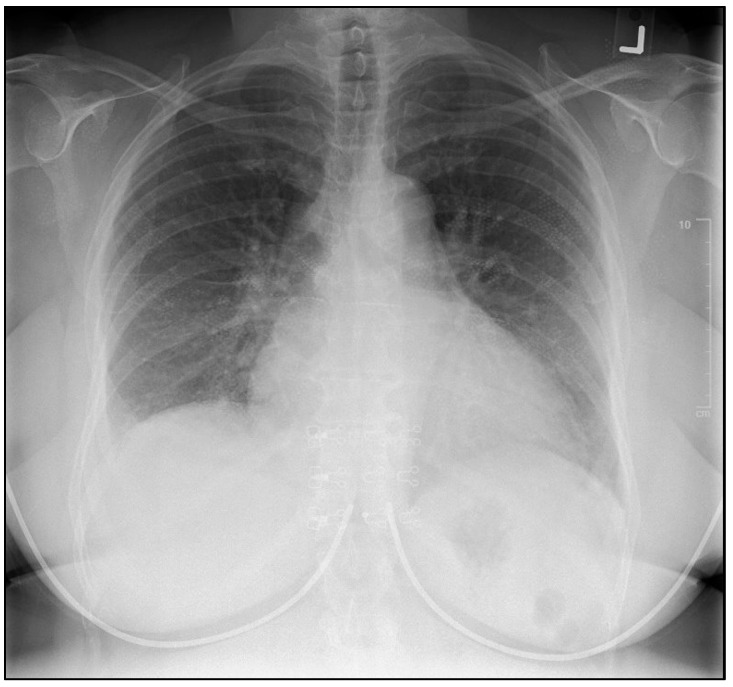
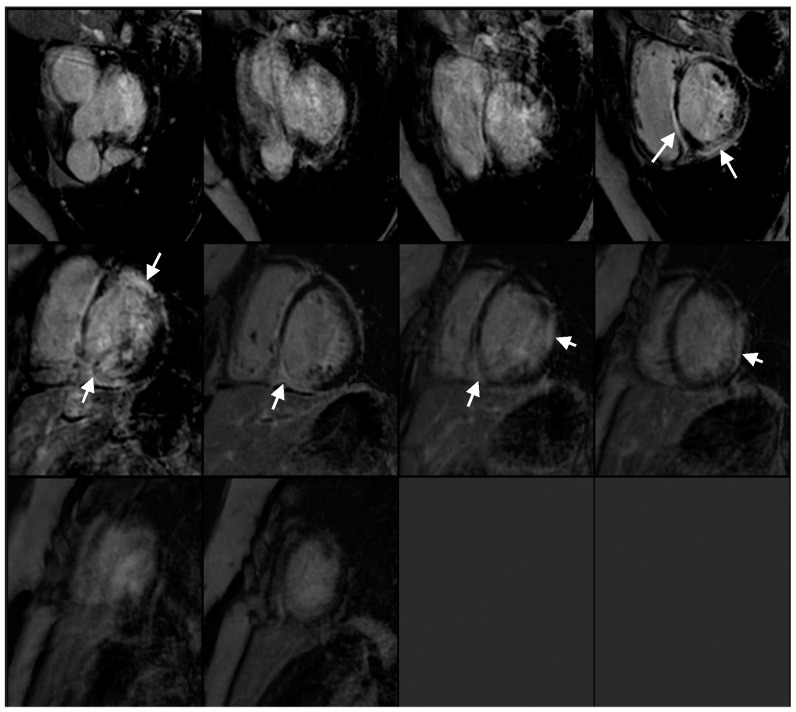
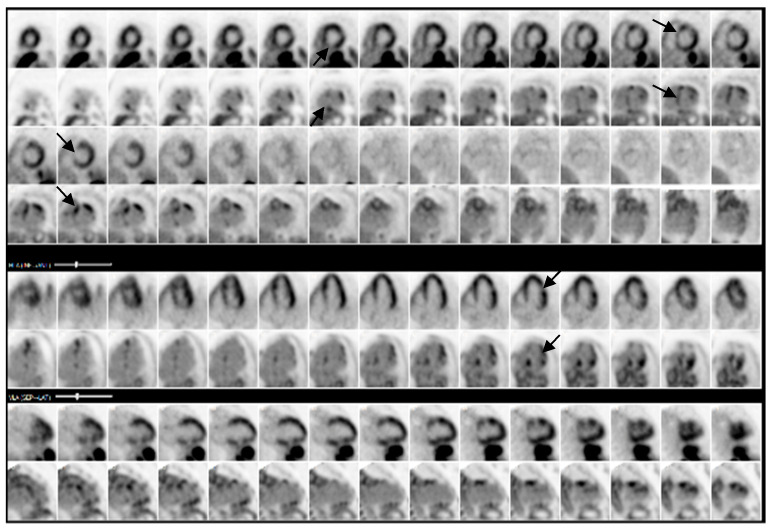
Cardiac sarcoidosis (CS) is a rare but life-threatening disorder, occurring in 2-5% of sarcoidosis cases, though post-mortem studies suggest a higher prevalence. It presents diagnostic challenges due to nonspecific symptoms and the low sensitivity of an endomyocardial biopsy. Recent guidelines emphasize multimodal imaging, such as cardiac magnetic resonance imaging (MRI) and positron emission tomography (PET). Given the risk of heart failure (HF) and arrhythmias, early detection is critical. This case highlights the role of non-invasive imaging in diagnosing CS and guiding treatment. A 54-year-old female with asthma, hyperlipidemia, a recent diagnosis of anterior uveitis, and familial sarcoidosis presented with dyspnea, chest tightness, and worsening cough. Examination revealed anterior uveitis, erythema nodosum, jugular venous distension, and pedal edema. The electrocardiogram (ECG) demonstrated bifascicular block and premature ventricular contractions (PVCs). The brain natriuretic peptide (BNP) was 975 pg/mL, with the transthoracic echocardiogram revealing a left ventricular ejection fraction of 25-30% with global LV akinesis. Coronary computed tomography angiography (CCTA) excluded coronary artery disease. Cardiac MRI showed late gadolinium enhancement, with PET demonstrating active myocardial inflammation, supporting a >90% probability of CS. Given her clinical trajectory and risk of further decompensation, immunosuppressive therapy was initiated without pursuing a biopsy. A dual-chamber implantable cardioverter defibrillator (ICD) was placed due to risk of ventricular arrhythmias. Bronchoalveolar lavage (BAL) showed a CD4/CD8 ratio of 6.53, reinforcing the diagnosis. She responded well to treatment, with symptom improvement and repeat imaging demonstrating signs of disease remission. This case underscores the growing role of multimodal imaging in CS diagnosis, potentially replacing biopsy in select cases. Early imaging-based diagnosis enabled timely immunosuppression and ICD placement, improving outcomes.
心脏结节病(CS)是一种罕见但危及生命的疾病,在2%至5%的结节病病例中出现,不过尸检研究表明其患病率更高。由于症状不具特异性以及心内膜活检敏感性较低,它带来了诊断挑战。近期指南强调多模态成像,如心脏磁共振成像(MRI)和正电子发射断层扫描(PET)。鉴于存在心力衰竭(HF)和心律失常的风险,早期检测至关重要。本病例突出了非侵入性成像在诊断CS和指导治疗中的作用。一名54岁女性,患有哮喘、高脂血症,近期诊断为前葡萄膜炎,并有家族性结节病,出现呼吸困难、胸闷和咳嗽加重症状。检查发现前葡萄膜炎、结节性红斑、颈静脉扩张和足部水肿。心电图(ECG)显示双分支阻滞和室性早搏(PVCs)。脑钠肽(BNP)为975 pg/mL,经胸超声心动图显示左心室射血分数为25%至30%,左心室整体运动减弱。冠状动脉计算机断层扫描血管造影(CCTA)排除了冠状动脉疾病。心脏MRI显示钆延迟强化,PET显示有活动性心肌炎症,支持CS的可能性大于90%。鉴于她的临床病程以及进一步失代偿的风险,未进行活检即开始免疫抑制治疗。由于存在室性心律失常风险,植入了双腔植入式心脏复律除颤器(ICD)。支气管肺泡灌洗(BAL)显示CD4/CD8比值为6.53,进一步支持了诊断。她对治疗反应良好,症状改善,重复成像显示疾病缓解迹象。本病例强调了多模态成像在CS诊断中日益重要的作用,在某些情况下可能取代活检。基于成像的早期诊断能够及时进行免疫抑制治疗和植入ICD,改善治疗结果。