Katsnelson Beatrice M, Rancu Albert L, Winter Adam D, Jonnalagadda Anshu, Smith-Voudouris Julian, Grauer Jonathan N
Department of Orthopaedics and Rehabilitation, Yale School of Medicine, New Haven, CT, USA.
N Am Spine Soc J. 2025 Jun 30;23:100765. doi: 10.1016/j.xnsj.2025.100765. eCollection 2025 Sep.
Postoperative adverse events following lumbar discectomy (LD) are important to characterize for patient counseling and risk management, particularly in potentially vulnerable patient populations, such as those with sleep apnea (SA). Although increasing screening and optimization pathways are starting to be put into place for patients with SA in general, specific attention to this condition in relation to LD has not been reported.
Adult patients undergoing isolated, single-level, lumbar laminotomy/discectomy were identified from the 2010 to 2022 PearlDiver Mariner database. Those without versus with SA were matched 4:1 based on age, sex, and Elixhauser comorbidity index (ECI). Ninety-day severe and minor adverse events, emergency department (ED) visits, and readmissions were assessed and compared with multivariate analysis. Overall 90-day reimbursements and 5-year revisions were assessed and compared.
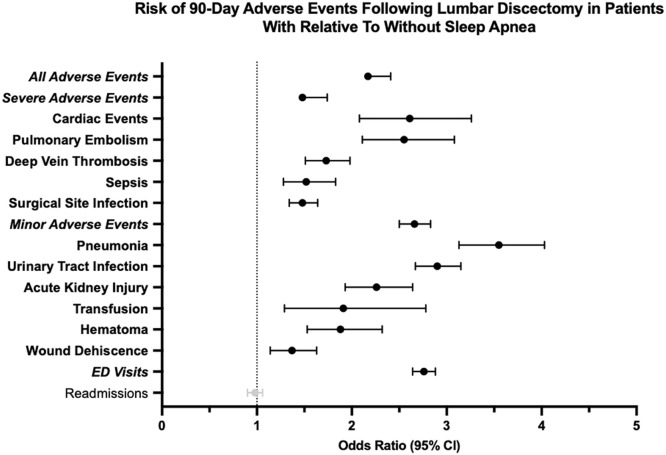
Of a total of 200,515 LD patient, SA was identified for 24,975 (12.5%). After matching, there were 74,391 without sleep apnea and 18,734 with sleep apnea. Patients with SA had independently higher odds-ratio (OR) of experiencing most 90-day postoperative adverse events, as well as aggregated severe (OR: 1.60) and minor (OR: 2.66) adverse events (p<.0001 for each). Patients with SA were also at higher odds of 90-day ED visits (OR: 2.76) and median overall 90-day reimbursement ($3,300.00 vs.. $3,106.00) (p<.0001 for both). Further, patients with SA were more likely to undergo 5-year subsequent lumbar surgery (p=.01).
While increasing attention has been given to SA around surgical interventions, the current study defined that over a tenth of LD patients had diagnosed SA and were at greater odds of severe and minor adverse events, as well as reoperations, in their postoperative period. This translated to greater health care utilization and cost. Consequently, patients with SA ought to receive supplemental risk counseling and postoperative resource planning when considered for LD.
腰椎间盘切除术(LD)后的术后不良事件对于患者咨询和风险管理非常重要,特别是在潜在脆弱的患者群体中,如患有睡眠呼吸暂停(SA)的患者。尽管针对一般SA患者的筛查和优化途径开始逐步实施,但尚未有关于LD与这种情况的具体关注的报道。
从2010年至2022年的PearlDiver Mariner数据库中识别接受孤立、单节段腰椎板切开术/椎间盘切除术的成年患者。根据年龄、性别和埃利克斯豪泽合并症指数(ECI),将无SA与有SA的患者按4:1进行匹配。评估90天内的严重和轻微不良事件、急诊科(ED)就诊情况和再入院情况,并通过多变量分析进行比较。评估并比较总体90天的报销情况和5年的翻修情况。
在总共200,515例LD患者中,确诊SA的有24,975例(12.5%)。匹配后,无睡眠呼吸暂停的患者有74,391例,有睡眠呼吸暂停的患者有18,734例。SA患者在术后90天发生大多数不良事件以及严重(比值比[OR]:1.60)和轻微(OR:2.66)不良事件的独立比值比更高(每项p<0.0001)。SA患者90天内ED就诊的几率也更高(OR:2.76),总体90天报销中位数也更高(3300.00美元对3106.00美元)(两者p<0.0001)。此外,SA患者更有可能在5年后接受腰椎再次手术(p = 0.01)。
虽然围绕手术干预对SA的关注日益增加,但当前研究表明,超过十分之一的LD患者被诊断患有SA,并且在术后发生严重和轻微不良事件以及再次手术的几率更高。这导致了更高的医疗保健利用率和成本。因此,在考虑为SA患者进行LD时,他们应该接受补充风险咨询和术后资源规划。