Samanta Ajanta, Bera Riya, Barua Medha, Debbarma Durlabh, Pande Arindam
Obstetrics and Gynecology, R. G. Kar Medical College and Hospital, Kolkata, IND.
Cardiology, Medica SuperSpecialty Hospital, Kolkata, IND.
Cureus. 2025 Jul 2;17(7):e87156. doi: 10.7759/cureus.87156. eCollection 2025 Jul.
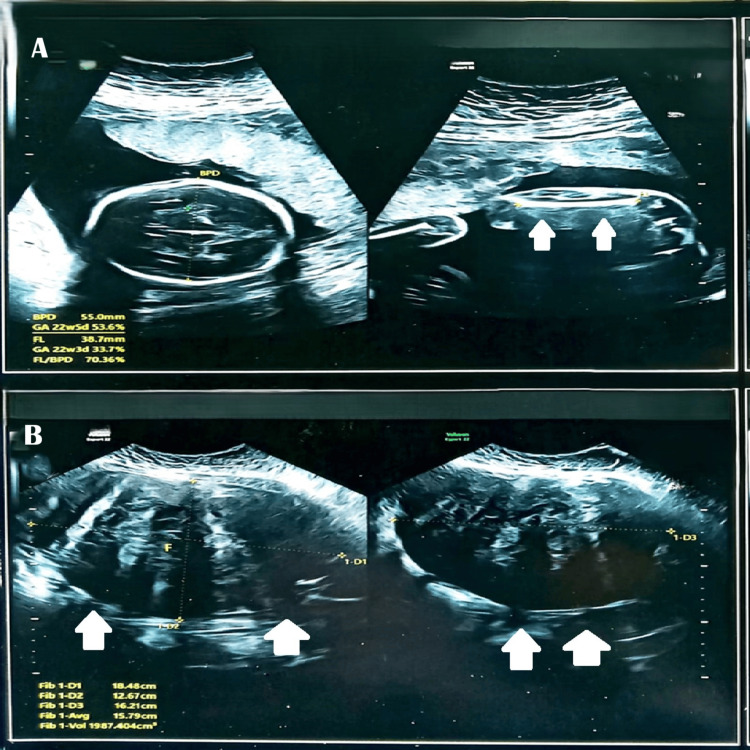
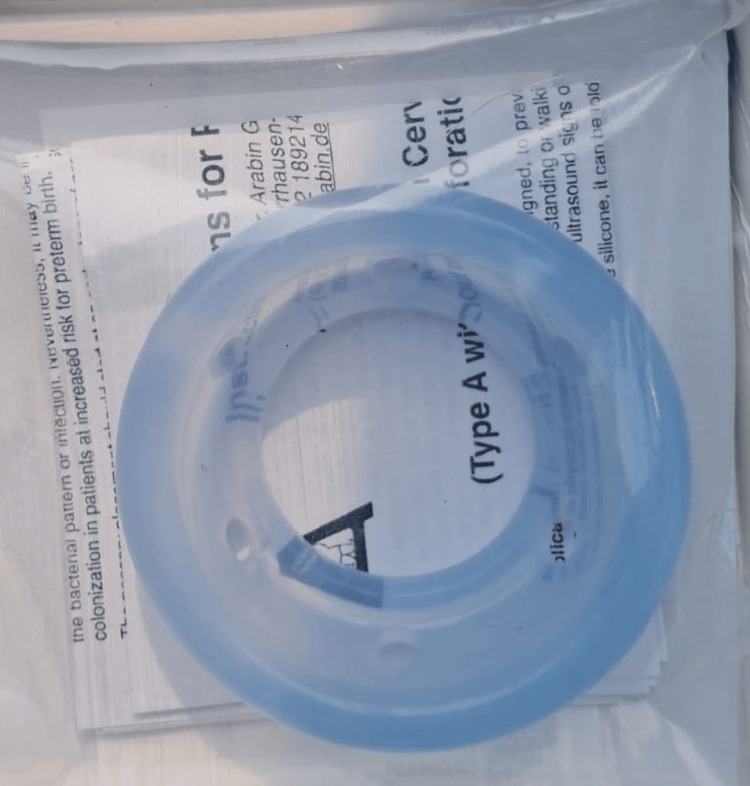
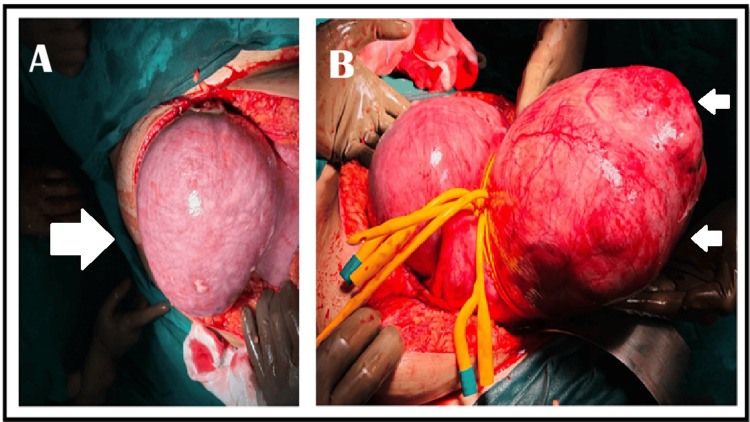
Uterine torsion during pregnancy is a rare and life-threatening condition that is frequently misdiagnosed due to nonspecific symptoms and imaging limitations. This case report describes a 32-year-old third gravida (G3, P0+2) with recurrent pregnancy loss, having a 16.9 cm uterine fibroid and hypertrophic cardiomyopathy (managed with bisoprolol), who presented at 24 weeks with severe abdominal pain. Although her vitals were stable, a markedly elevated C-reactive protein (CRP) (245 mg/dL) raised concern for acute pathology. Initial ultrasound incorrectly localized the fibroid to the left, but exploratory laparotomy revealed a 180-degree uterine torsion with contralateral fibroid position, revising the diagnosis from fibroid degeneration to this rare emergency, leading to detorsion and myomectomy. At 30 weeks' gestation, cervical insufficiency (a short cervix measuring 0.5 cm with funneling) was successfully managed with an Arabin pessary and weekly 500 mg injections of hydroxyprogesterone, prolonging the pregnancy to 34 weeks and resulting in an outlet forceps delivery of a healthy 1.9 kg infant. This case highlights the importance of surgical exploration when clinical suspicion contradicts imaging findings, the feasibility of pregnancy-preserving surgery for uterine torsion, and the effectiveness of combined mechanical-hormonal therapy for cervical insufficiency following complex uterine interventions. Multidisciplinary care was critical to manage overlapping high-risk factors, including fibroids, cardiac disease, and preterm cervical changes, ultimately leading to a favorable outcome.
妊娠期子宫扭转是一种罕见且危及生命的疾病,由于症状不具特异性和影像学检查存在局限性,常被误诊。本病例报告描述了一名32岁的经产妇(G3,P0+2),有复发性流产史,患有16.9厘米的子宫肌瘤和肥厚型心肌病(服用比索洛尔治疗),在孕24周时出现严重腹痛。尽管她的生命体征稳定,但显著升高的C反应蛋白(CRP)(245毫克/分升)引发了对急性病变的担忧。最初的超声检查错误地将肌瘤定位在左侧,但剖腹探查发现子宫扭转180度,肌瘤位于对侧,从而将诊断从肌瘤变性改为这种罕见的急症,随后进行了子宫复位和肌瘤切除术。在妊娠30周时,成功地使用了阿拉宾子宫托并每周注射500毫克羟孕酮治疗宫颈机能不全(宫颈短,长度为0.5厘米且有漏斗状改变),将妊娠延长至34周,并通过出口产钳助产分娩出一名健康的1.9千克婴儿。本病例强调了在临床怀疑与影像学检查结果相矛盾时进行手术探查的重要性、子宫扭转保留妊娠手术的可行性,以及复杂子宫干预后机械 - 激素联合治疗宫颈机能不全的有效性。多学科护理对于管理包括肌瘤、心脏病和早产宫颈改变在内的重叠高危因素至关重要,最终带来了良好的结局。