Chen I-Wen, Huang Chung-Huei, Liu Pi-Hua, Lin Cheng-Wei, Hung Shih-Yuan, Huang Yu-Yao
Department of Endocrinology and Metabolism, Chang Gung Memorial Hospital, Taoyuan City, Taiwan.
College of Medicine, Chang Gung University, Taoyuan City, Taiwan.
Therap Adv Gastroenterol. 2025 Jul 31;18:17562848251356198. doi: 10.1177/17562848251356198. eCollection 2025.
Chronic viral hepatitis is a major risk factor for hepatocellular carcinoma (HCC). Though diabetes is another risk of HCC, it remains indeterminant as to whether glycemic burden in individuals with type 2 diabetes (T2D) should be differentially managed according to the presence of chronic hepatitis B virus (HBV) or hepatitis C virus (HCV).
To evaluate the association between glycemic burden and HCC risk in individuals with T2D, stratified by viral hepatitis status, including HBV and HCV.
Retrospective cohort study.
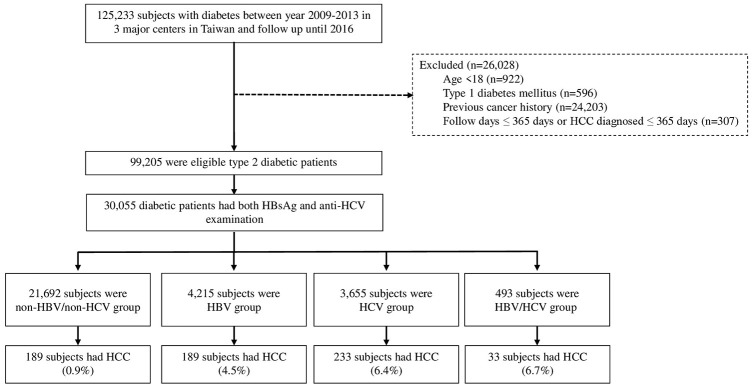
This study analyzed 30,055 individuals with T2D from the Chang Gung Research Database (2009-2016), stratified into non-HBV/non-HCV, HBV, and HCV groups. Glycemic burden was assessed using baseline glycated hemoglobin (HbA1c), high HbA1c variability, and optimal glycemic control, defined as maintaining HbA1c <7% for more than 80% of the follow-up period. Cox proportional hazard models were used to identify HCC risk factors.
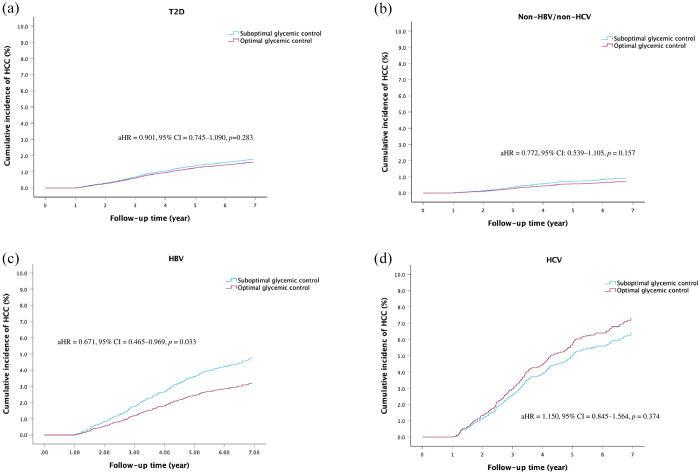
Over a mean follow-up of 6.4 years, 644 individuals (2.14%) developed HCC. Viral hepatitis was the predominant independent risk factor, followed by elevated fibrosis-4 (FIB-4) scores, male sex, older age, low albumin, and low platelet count. Neither baseline HbA1c nor high HbA1c variability was associated with HCC risk in the overall T2D population or stratified groups. However, optimal glycemic control was significantly associated with reduced HCC risk in individuals with HBV (adjusted hazard ratio (HR) = 0.671, 95% confidence interval (CI) = 0.465-0.969, = 0.033) and demonstrated a potentially beneficial role in non-HBV/non-HCV patients with presumed metabolic dysfunction-associated fatty liver disease (presumed MAFLD; adjusted HR = 0.574, 95% CI: 0.309-1.065, = 0.079).
Optimal glycemic control may reduce HCC risk in individuals with T2D and HBV and potentially benefits those with presumed MAFLD, although its role in HCV-related HCC appears limited. These findings highlight the need for tailored glycemic management strategies based on viral hepatitis type.
慢性病毒性肝炎是肝细胞癌(HCC)的主要危险因素。虽然糖尿病是HCC的另一个风险因素,但对于2型糖尿病(T2D)患者的血糖负担是否应根据慢性乙型肝炎病毒(HBV)或丙型肝炎病毒(HCV)的存在进行差异化管理仍不确定。
评估T2D患者中血糖负担与HCC风险之间的关联,并根据病毒性肝炎状态(包括HBV和HCV)进行分层。
回顾性队列研究。
本研究分析了长庚研究数据库(2009 - 2016年)中的30,055名T2D患者,分为非HBV/非HCV、HBV和HCV组。使用基线糖化血红蛋白(HbA1c)、高HbA1c变异性和最佳血糖控制来评估血糖负担,最佳血糖控制定义为在随访期的80%以上维持HbA1c<7%。采用Cox比例风险模型确定HCC风险因素。
在平均6.4年的随访中,644名个体(2.14%)发生了HCC。病毒性肝炎是主要的独立危险因素,其次是纤维化-4(FIB-4)评分升高、男性、年龄较大、白蛋白水平低和血小板计数低。在总体T2D人群或分层组中,基线HbA1c和高HbA1c变异性均与HCC风险无关。然而,最佳血糖控制与HBV患者的HCC风险降低显著相关(调整后风险比(HR)=0.671,95%置信区间(CI)=0.465 - 0.969,P = 0.033),并且在假定患有代谢功能障碍相关脂肪性肝病(假定MAFLD)的非HBV/非HCV患者中显示出潜在的有益作用(调整后HR = 0.574,95% CI:0.309 - 1.065,P = 0.079)。
最佳血糖控制可能降低T2D和HBV患者的HCC风险,并可能使假定患有MAFLD的患者受益,尽管其在HCV相关HCC中的作用似乎有限。这些发现凸显了基于病毒性肝炎类型制定个性化血糖管理策略的必要性。