Department of Medicine, Yale School of Medicine, New Haven, Connecticut.
Department of Medicine, Veterans Affairs Connecticut Healthcare, West Haven, Connecticut.
JAMA Netw Open. 2024 Nov 4;7(11):e2443608. doi: 10.1001/jamanetworkopen.2024.43608.
Hepatocellular carcinoma (HCC) is typically detected only at advanced stages when treatment options are limited. Most of the current HCC risk models focus on patients with viral hepatitis or diagnosed cirrhosis or require variables not routinely available in clinical care.
To identify modifiable HCC risk factors in the general population and to develop a risk score to inform HCC screening and risk-factor modification interventions for high-risk individuals without viral hepatitis or decompensated cirrhosis.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study analyzed demographic, clinical, laboratory, and diagnostic data from the US Department of Veterans Affairs (VA) electronic health records. Data were divided into development and validation samples. Veterans aged 30 to 95 years were included, and those with hepatitis B or C virus infection, hepatic decompensation, or prevalent HCC were excluded. Patients were followed up until the occurrence of HCC diagnosis, death, or December 31, 2021. A Cox proportional hazards regression model for 10-year risk of HCC was developed and used to create an HCC risk score, and performance in development and validation samples and in patient subgroups was evaluated. One outpatient visit date per person at least 18 months after VA entry, between October 1, 2007, and March 31, 2020, was randomly selected and used as the index date for the start of follow-up. Analyses were performed from March 2023 to May 2024.
Age, sex, race and ethnicity, body mass index, liver fibrosis (detected with Fibrosis-4 Index [FIB-4]), diabetes status, smoking status, and alcohol use.
First HCC diagnosis during follow-up. This information was ascertained from VA national cancer registry topography and histology codes and from International Classification of Diseases, Ninth Revision and International Statistical Classification of Diseases, Tenth Revision, Clinical Modification diagnosis codes for the inpatient or outpatient visits.
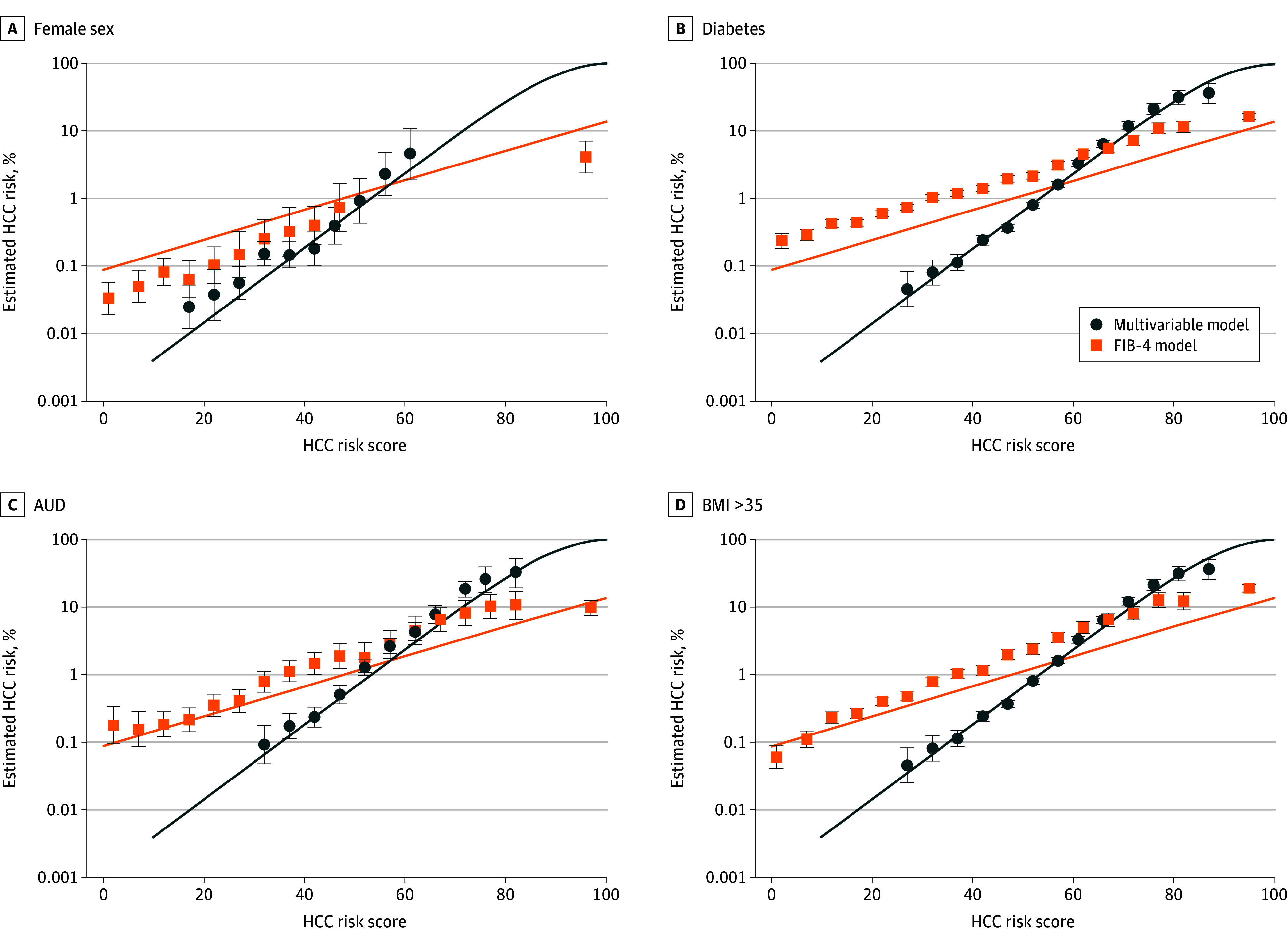
This study of 6 509 288 veterans included 6 048 917 males (92.9%), with a median (IQR) age of 65 (54-74) years, who identified as being of Hispanic (5.3%), non-Hispanic Black (15.0%), non-Hispanic White (68.9%), or other (4.6%) race and ethnicity. Overall, 15 142 patients (0.2%) developed HCC, 69.5% of whom had FIB-4 of 3.25 or lower at baseline. While FIB-4 was the most important variable, age, sex, race and ethnicity, body mass index, diabetes, smoking, and alcohol use were also informative. Discrimination in the development sample was better than FIB-4 alone (C statistic, 0.83 [95% CI, 0.82-0.85] vs 0.79 [95% CI, 0.77-0.80]). The HCC risk score performed consistently well in the validation sample and in all subgroups. A FIB-4 threshold of 3.25 would screen 5.0% of the cohort at a cost of 28 false-positives for every true-positive; a model risk score of 58 would screen 4.7% of the cohort at a cost of 23 false-positives for every true-positive.
Results of this study suggest that a multivariable risk score that uses routinely available clinical data outperforms FIB-4 alone in identifying patients at risk of HCC who do not have viral hepatitis or hepatic decompensation at baseline.
肝细胞癌(HCC)通常仅在治疗选择有限的晚期阶段才能被检测到。目前大多数 HCC 风险模型主要针对患有病毒性肝炎或诊断为肝硬化的患者,或需要常规临床护理中不可用的变量。
确定一般人群中可改变的 HCC 风险因素,并开发一种风险评分,以告知无病毒性肝炎或失代偿性肝硬化的高危人群进行 HCC 筛查和风险因素修正干预。
设计、地点和参与者:这项队列研究分析了美国退伍军人事务部(VA)电子健康记录中的人口统计学、临床、实验室和诊断数据。数据分为开发和验证样本。纳入年龄在 30 至 95 岁之间的退伍军人,排除乙型或丙型肝炎病毒感染、肝失代偿或现患 HCC 的患者。患者随访至 HCC 诊断、死亡或 2021 年 12 月 31 日。为 10 年 HCC 风险开发了 Cox 比例风险回归模型,并用于创建 HCC 风险评分,并评估了开发和验证样本以及患者亚组中的表现。在 2007 年 10 月 1 日至 2020 年 3 月 31 日期间,从 VA 进入后的至少 18 个月内随机选择每人的一次门诊就诊日期,并将其用作随访开始的索引日期。分析于 2023 年 3 月至 2024 年 5 月进行。
年龄、性别、种族和民族、体重指数、肝纤维化(通过 Fibrosis-4 Index [FIB-4] 检测)、糖尿病状况、吸烟状况和饮酒状况。
随访期间的首次 HCC 诊断。这些信息是从 VA 国家癌症登记处的地形学和组织学代码以及国际疾病分类、第九版和国际疾病分类、第十版临床修正的住院或门诊就诊的诊断代码中确定的。
这项对 6509288 名退伍军人的研究包括 6048917 名男性(92.9%),中位(IQR)年龄为 65(54-74)岁,他们的种族和民族身份为西班牙裔(5.3%)、非西班牙裔黑人(15.0%)、非西班牙裔白人(68.9%)或其他(4.6%)。总体而言,有 15142 名患者(0.2%)患有 HCC,其中 69.5%的患者在基线时 FIB-4 为 3.25 或更低。虽然 FIB-4 是最重要的变量,但年龄、性别、种族和民族、体重指数、糖尿病、吸烟和饮酒也是有用的。在开发样本中的区分能力优于 FIB-4 单独使用(C 统计量,0.83 [95%CI,0.82-0.85] vs 0.79 [95%CI,0.77-0.80])。HCC 风险评分在验证样本和所有亚组中表现一致良好。FIB-4 阈值为 3.25 将以每 28 个假阳性检测到 5.0%的队列,而模型风险评分 58 将以每 23 个假阳性检测到 4.7%的队列。
这项研究的结果表明,一种使用常规临床数据的多变量风险评分在识别没有基线病毒性肝炎或肝失代偿的 HCC 高危人群方面优于 FIB-4 单独使用。