Landsberg Adina, Brockman Nicole K, Sevinc Emir, McClurg Caitlin, Elliott Meghan J, Girard Louis-Philippe, James Matthew T, Leung Alexander A, Pannu Neesh I, Pasternak Meghann, Ronksley Paul E, Tonelli Marcello, Harrison Tyrone G
Department of Medicine, University of Calgary, AB, Canada.
Libraries and Cultural Resources, University of Calgary, AB, Canada.
Can J Kidney Health Dis. 2025 Jul 29;12:20543581251358144. doi: 10.1177/20543581251358144. eCollection 2025.
People with advanced chronic kidney disease (CKD) and secondary hyperparathyroidism (sHPT) refractory to medical therapy often require surgical parathyroidectomy. Severe and prolonged hypocalcemia immediately following parathyroidectomy for sHPT is often termed "hungry bone syndrome" (HBS).
To systematically review the effect of pre-operative interventions on post-operative hypocalcemia, HBS, and other related outcomes in patients with CKD and sHPT undergoing parathyroidectomy.
This is a systematic review study.
Diverse study designs conducted in any country.
Adult patients with CKD complicated by sHPT undergoing parathyroidectomy.
Post-operative hypocalcemia, HBS, symptomatic hypocalcemia, and other related outcomes.
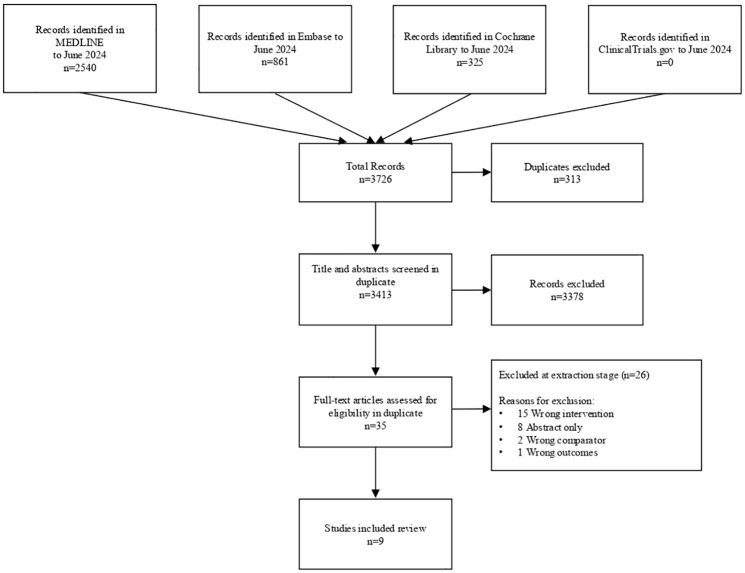
We searched Ovid MEDLINE, Embase, and Cochrane Controlled Trials Registry from inception until June 2024 for trials and observational studies of adults with CKD and sHPT that evaluated pre-operative interventions aimed at reducing the risk of hypocalcemia following parathyroidectomy. After 2 phases of study screening conducted in duplicate, we extracted data on study design, patient characteristics, interventions, and outcomes. Hypocalcemia was defined as serum calcium <2.1 mmol/L and HBS as calcium <2.1 mmol/L for ≥4 days post-operatively. We evaluated the risk of bias and completed a narrative synthesis of the available literature across intervention types.
We identified 3616 studies; 35 underwent full-text review, and 9 met final eligibility criteria. Interventions included pre-operative calcitriol (n = 2), pre-operative cinacalcet (n = 3), pre-operative alkaline phosphatase (ALP) measurement to guide intravenous (IV) calcium administration (n = 3), and pre-operative pamidronate (n = 1). All studies reported on at least one of: median/mean post-operative calcium (n = 7), incidence of post-operative hypocalcemia (n = 3), HBS (n = 1), and symptomatic hypocalcemia (n = 4). Interventions that reported on the risk of post-operative hypocalcemia included pre-operative pamidronate (n = 1, 37 participants, odds ratio [OR] = 0.003, 95% confidence interval [CI] = 0.000-0.072) and IV calcium guided by pre-operative ALP (n = 1, 271 participants, OR = 0.292, 95% CI = 0.175-0.488). There were insufficient data to meta-analyze study-specific effects for any intervention or outcome.
Our study was limited by significant heterogeneity in outcome reporting, which resulted in substantial outcome reporting bias and prevented pooled analyses. Furthermore, no randomized control trials met our inclusion criteria, which limited assessment of publication bias.
Pre-operative risk factors for HBS have been established in patients with CKD undergoing parathyroidectomy. However, limited research has evaluated pre-operative interventions to reduce the risk of HBS, and due to heterogeneity in outcome reporting across studies, there is still uncertainty about the effectiveness of such interventions. These findings support the need for future clinical trials.
患有晚期慢性肾脏病(CKD)且对药物治疗难治的继发性甲状旁腺功能亢进(sHPT)患者通常需要进行甲状旁腺切除术。因sHPT行甲状旁腺切除术后立即出现的严重且持续时间较长的低钙血症通常被称为“饥饿骨综合征”(HBS)。
系统评价术前干预措施对接受甲状旁腺切除术的CKD和sHPT患者术后低钙血症、HBS及其他相关结局的影响。
这是一项系统评价研究。
在任何国家开展的多种研究设计。
患有CKD并合并sHPT且接受甲状旁腺切除术的成年患者。
术后低钙血症、HBS、症状性低钙血症及其他相关结局。
我们检索了Ovid MEDLINE、Embase和Cochrane对照试验注册库,从建库至2024年6月,查找关于患有CKD和sHPT的成年人的试验和观察性研究,这些研究评估了旨在降低甲状旁腺切除术后低钙血症风险的术前干预措施。在进行两轮重复的研究筛选后,我们提取了关于研究设计、患者特征、干预措施和结局的数据。低钙血症定义为血清钙<2.1 mmol/L,HBS定义为术后≥4天血清钙<2.1 mmol/L。我们评估了偏倚风险,并对各类干预措施的现有文献进行了叙述性综合分析。
我们共识别出3616项研究;35项进行了全文审查,9项符合最终纳入标准。干预措施包括术前骨化三醇(n = 2)、术前西那卡塞(n = 3)、术前测量碱性磷酸酶(ALP)以指导静脉注射钙剂(n = 3)以及术前帕米膦酸盐(n = 1)。所有研究均报告了以下至少一项:术后钙的中位数/平均值(n = 7)、术后低钙血症的发生率(n = 3)、HBS(n = 1)以及症状性低钙血症(n = 4)。报告了术后低钙血症风险的干预措施包括术前帕米膦酸盐(n = 1,37名参与者,比值比[OR]=0.003,95%置信区间[CI]=0.000 - 0.072)以及术前ALP指导下的静脉注射钙剂(n = 1,271名参与者,OR = 0.292,95% CI = 0.175 - 0.488)。没有足够的数据对任何干预措施或结局进行特定研究效应的荟萃分析。
我们的研究受到结局报告中显著异质性的限制,这导致了大量的结局报告偏倚,并妨碍了汇总分析。此外,没有随机对照试验符合我们的纳入标准,这限制了对发表偏倚的评估。
已确定接受甲状旁腺切除术的CKD患者中HBS的术前危险因素。然而,评估降低HBS风险的术前干预措施的研究有限,并且由于各研究结局报告的异质性,此类干预措施的有效性仍存在不确定性。这些发现支持未来进行临床试验的必要性。