Ramatla Tsepo, Nkhebenyane Jane, Lekota Kgaugelo E, Thekisoe Oriel, Monyama Maropeng, Achilonu Conrad Chibunna, Khasapane George
Centre for Applied Food Safety and Biotechnology, Department of Life Sciences, Central University of Technology, Bloemfontein, South Africa.
Unit for Environmental Sciences and Management, North-West University, Potchefstroom, South Africa.
Front Microbiol. 2025 Jul 21;16:1599070. doi: 10.3389/fmicb.2025.1599070. eCollection 2025.
Carbapenem-resistant (CRPA) represents a global threat, but the global distribution of carbapenem resistant bacteria remains a critical issue in public health.
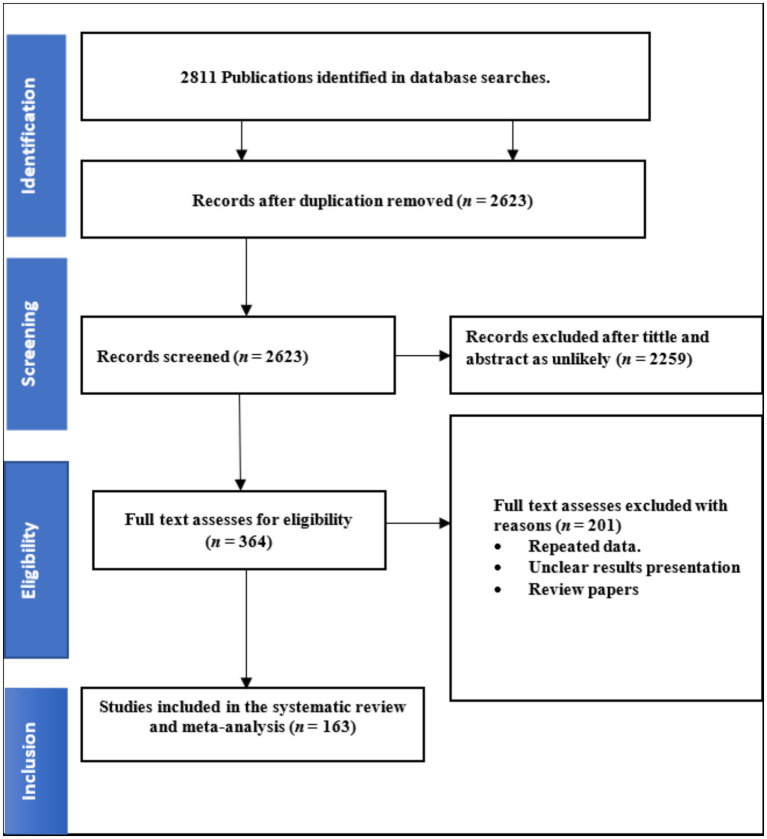
We conducted a systematic review and meta-analysis on the global pooled prevalence estimate (PPE) of CRPA and their antibiotic resistance. The systematic review protocol was registered with PROSPERO (CRD42024579654). This study was carried out following the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. Heterogeneity between studies was assessed using Cochrane Q test and I test statistics based on the random effects model. Comprehensive meta-analysis software v4.0 was used to analyze the pooled prevalence of CRPA.
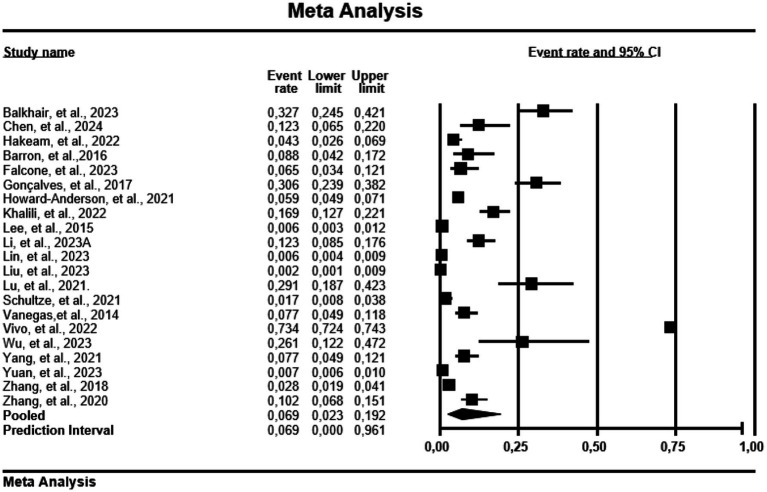
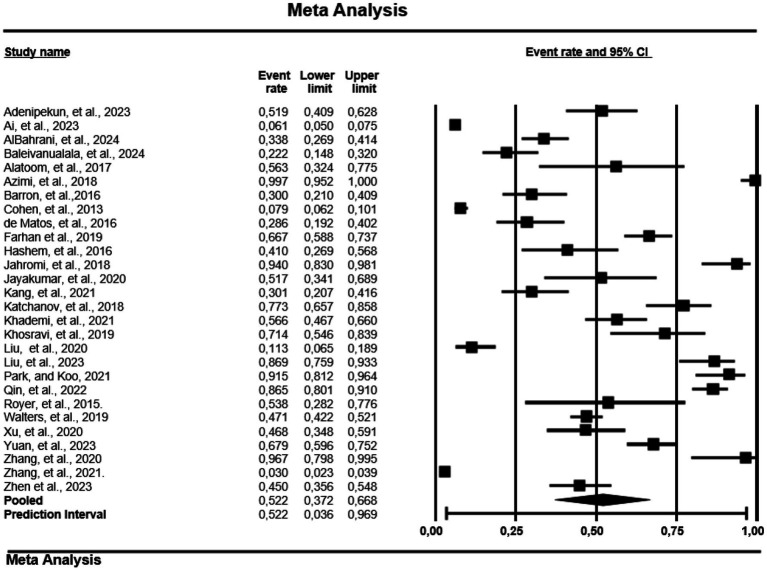
A total of 163 studies (both clinical and screening samples) containing a total of 58,344 cases from 39 countries were included in this study. The overall PPE of CRPA was 34.7% (95% CI: 0.316-0.37.8) for both clinical and screening samples. Meropenem had a PPE of 31.2% (95% CI: 0.272-0.352) and imipenem had the lowest PPE of 27.7% (95% CI: 0.238-0.319). Japan had the highest PPE at 98.2% (95% CI: 0.482-0.100) of CRPA, and the lowest was observed for Saudi Arabia at 13.9% (95% CI: 0. 064-0. 277). CRPA is widespread on five continents except Australia and Antarctica, while the highest PPE is in Europe at 47.6% (95% CI: 0.359-0.595) and the lowest in Asia at 32, 8% (95% CI: 0.293-0.364). The relatively higher PPE of CRPA was observed in Europe during the year interval 2014-2017 at 95.4% (95% CI: 0.388-0.999), followed by Africa from the year 2022-2024 with 38.5% (95% CI: 0.243-0.550). Ceftazidime was significantly higher in studies conducted before 2019 with a PPE of 44.7% (95% CI: 0.246% - 0.668), while CRPA after 2019 had a higher resistance to cefoperazone/sulbactam with a PPE of 17.3% (95% CI: 0.050-0.455).
This review indicates that the prevalence of CRPA is generally high and varies significantly between countries. To prevent the emergence of CRPA and antibiotic resistance, future initiatives should prioritise strengthening laboratory capacity for early detection of antibiotic resistance.
耐碳青霉烯类(CRPA)是一个全球性威胁,但耐碳青霉烯类细菌的全球分布仍是公共卫生领域的一个关键问题。
我们对CRPA的全球合并流行率估计(PPE)及其抗生素耐药性进行了系统评价和荟萃分析。该系统评价方案已在PROSPERO(CRD42024579654)注册。本研究按照系统评价和荟萃分析的首选报告项目(PRISMA)指南进行。采用Cochrane Q检验和基于随机效应模型的I检验统计量评估研究间的异质性。使用综合荟萃分析软件v4.0分析CRPA的合并流行率。
本研究共纳入163项研究(临床样本和筛查样本),涵盖来自39个国家的58344例病例。临床样本和筛查样本中CRPA的总体PPE为34.7%(95%CI:0.316 - 0.378)。美罗培南(PPE为31.2%,95%CI:0.272 - 0.352),亚胺培南的PPE最低,为27.7%(95%CI:0.238 - 0.319)。日本CRPA的PPE最高,为98.2%(95%CI:0.482 - 0.100),沙特阿拉伯最低,为13.9%(95%CI:0.064 - 0.277)。除澳大利亚和南极洲外,CRPA在五大洲广泛存在,其中欧洲的PPE最高,为47.6%(95%CI:0.359 - 0.595),亚洲最低,为32.8%(95%CI:0.293 - 0.364)。在2014 - 2017年期间,欧洲CRPA的PPE相对较高,为95.4%(95%CI:0.388 - 0.999),其次是2022 - 2024年的非洲,为38.5%(95%CI:0.243 - 0.550)。在2019年之前进行的研究中,头孢他啶的PPE显著更高,为44.7%(95%CI:0.246% - 0.668),而2019年后CRPA对头孢哌酮/舒巴坦的耐药性更高,PPE为17.3%(95%CI:0.050 - 0.455)。
本综述表明,CRPA的流行率普遍较高,且各国之间差异显著。为防止CRPA和抗生素耐药性的出现,未来的举措应优先加强早期检测抗生素耐药性的实验室能力。