Akdeniz Bayram Cevdet, Bahrami Shahram, Hagen Espen, Fuhrer Julian, Fominykh Vera, Shadrin Alexey, Filiz Tahir Tekin, Athanasiu Lavinia, Grenier-Boley Benjamin, Bellenguez Céline, de Rojas Itziar, Küçükali Fahri, Schneider Anja, Kleineidam Luca, Rujescu Dan, Scherbaum Norbert, Deckert Jürgen, Riedel-Heller Steffi, Hausner Lucrezia, Molina-Porcel Laura, Grimmer Timo, Heilmann-Heimbach Stefanie, Moebus Susanne, Scarmeas Nikolaos, García-Alberca Jose María, Franco-Macías Emilio, Mir Pablo, Real Luis M, Rodriguez-Rodriguez Eloy, Royo Jose Luís, Sáez María Eugenia, Carracedo Ángel, de Munain Adolfo Lopez, Amer-Ferrer Guillermo, Calero Miguel, Medina Miguel, Garcia-Ribas Guillermo, Mendioroz Maite, Dols-Icardo Oriol, Moreno Fermin, Pérez-Tur Jordi, Bullido María J, Álvarez Victoria, Soininen Hilkka, Heikkinen Sami, de Mendonça Alexandre, Mehrabian Shima, Traykov Latchezar, Hort Jakub, Vyhnalek Martin, Sandau Nicolai, Thomassen Jesper Qvist, Luo Jiao, Pijnenburg Yolande A L, Tesi Niccolo, van Swieten John, Giedraitis Vilmantas, Williams Julie, Nicolas Gael, Debette Stephanie, Amouyel Philippe, Grünblatt Edna, Popp Julius, Bossù Paola, Galimberti Daniela, Rossi Giacomina, Arosio Beatrice, Mecocci Patrizia, Squassina Alessio, Tremolizzo Lucio, Borroni Barbara, Nacmias Benedetta, Seripa Davide, Rainero Innocenzo, Daniele Antonio, Piras Fabrizio, Masullo Carlo, Kehoe Patrick Gavin, Frikke-Schmidt Ruth, Ghidoni Roberta, Ruiz Agustín, Fernandez Victoria, Sánchez-Juan Pascual, Sleegers Kristel, Ingelsson Martin, Hiltunen Mikko, Sims Rebecca, Ramirez Alfredo, Broce Iris J, Haavik Jan, Selbæk Geir, Knapskog Anne-Brita, Saltvedt Ingvild, Bergh Sverre, Aakhus Eivind, Kirsebom Bjørn-Eivind, Watne Leiv Otto, Rongve Arvid, Årsland Dag, Djurovic Srdjan, Stordal Eystein, Toft Mathias, Scheffler Katja, Fladby Tormod, Lambert Jean-Charles, Dale Anders, Frei Oleksandr, Andreassen Ole
Centre for Precision Psychiatry, Division of Mental Health and Addiction, Oslo University Hospital & Institute of Clinical Medicine, University of Oslo, Oslo, Norway.
Department of Pharmacy, Section for Pharmacology and Pharmaceutical Biosicences, University of Oslo, Oslo, Norway.
medRxiv. 2025 Jul 28:2025.07.28.25332293. doi: 10.1101/2025.07.28.25332293.
Polygenic hazard score (PHS) models can be used to predict the age-associated risk for complex diseases, including Alzheimer's disease (AD). In this study, we present an improved PHS model for AD that incorporates a large number of genetic variants and demonstrates enhanced predictive accuracy for age of onset in European populations compared to alternative models.
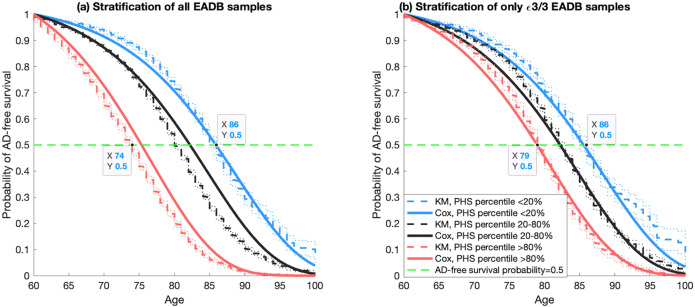
We used the genotyped European Alzheimer & Dementia Biobank (EADB) sample (n=42,120) to develop and evaluate the performance of the PHS model. We developed a PHS model building on 720 genetic variants, including Apolipoprotein E () ε2 and ε4 alleles. We used Elastic Net-regularized Cox regression approach to develop the PHS model.
The new PHS model (EADB720) improved prediction accuracy compared to alternative models in European populations, with the Odds Ratio OR from the highest quintile of risk (80th risk percentile and above) to the lowest quintile of risk (20th risk percentile and below) varying between 5.10 and 13.15 within the range of age of onset from 65 - 85 years. Our model also improved risk stratification across ε3/3 individuals of European ancestry (OR ranges from 1.95 to 3.52). It was also successfully validated in independent datasets (HUSK, DemGene and ADNI) by achieving OR80/20 up to 10.00 in each independent dataset.
Our EADB720 model significantly improves the accuracy of age-associated risk of AD across European populations (pval<0.03). Accurately predicting the age of onset of AD is of large clinical importance to implementing new AD medication and early intervention in clinical settings.
多基因风险评分(PHS)模型可用于预测包括阿尔茨海默病(AD)在内的复杂疾病与年龄相关的风险。在本研究中,我们提出了一种改进的AD的PHS模型,该模型纳入了大量基因变异,并且与其他模型相比,在欧洲人群中对发病年龄的预测准确性有所提高。
我们使用基因分型的欧洲阿尔茨海默病与痴呆生物样本库(EADB)样本(n = 42,120)来开发和评估PHS模型的性能。我们基于720个基因变异构建了一个PHS模型,包括载脂蛋白E()ε2和ε4等位基因。我们使用弹性网络正则化Cox回归方法来开发PHS模型。
与欧洲人群中的其他模型相比,新的PHS模型(EADB720)提高了预测准确性,在65 - 85岁的发病年龄范围内,风险最高五分位数(第80百分位数及以上)与风险最低五分位数(第20百分位数及以下)之间的优势比(OR)在5.10至13.15之间变化。我们的模型还改善了欧洲血统的ε3/3个体的风险分层(OR范围为1.95至3.52)。它在独立数据集(HUSK、DemGene和ADNI)中也成功得到验证,每个独立数据集中的OR80/20高达10.00。
我们的EADB720模型显著提高了欧洲人群中AD与年龄相关风险的预测准确性(p值<0.03)。准确预测AD的发病年龄对于在临床环境中实施新的AD药物治疗和早期干预具有重要的临床意义。