From the Biogen, Cambridge, MA.
Neurology. 2024 Feb 13;102(3):e207919. doi: 10.1212/WNL.0000000000207919. Epub 2023 Dec 28.
Amyloid-related imaging abnormalities (ARIA) were the most common adverse events reported in the phase 3 ENGAGE and EMERGE trials of aducanumab, an anti-amyloid monoclonal antibody. ε4 carrier status has been shown to increase risk of ARIA in prior trials of aducanumab and other anti-amyloid therapies; however, the remainder of the human genome has not been evaluated for ARIA risk factors. Therefore, we sought to determine in a hypothesis-free manner whether genetic variants beyond influence risk of ARIA in aducanumab-treated patients.
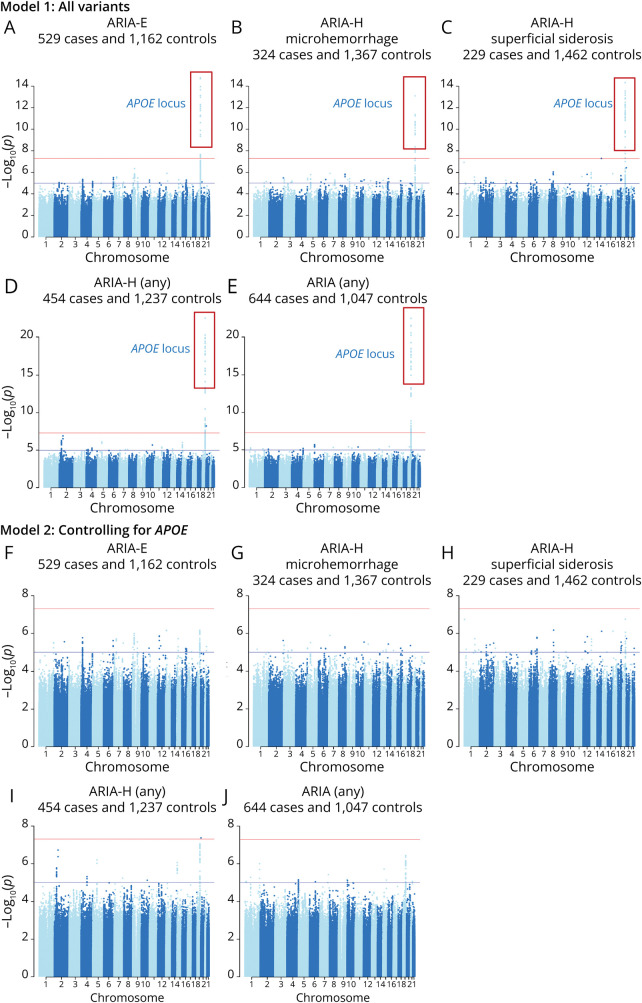
We performed genome-wide association studies (GWAS) of ARIA in participants in the ENGAGE and EMERGE trials. Participants had mild cognitive impairment due to Alzheimer disease or mild Alzheimer disease dementia and were amyloid-positive on PET scans. All participants underwent regular MRI monitoring to detect and diagnose ARIA.
Of the 3,285 participants in the intent-to-treat population, this analysis included 1,691 with genotyping array data who received at least one dose of aducanumab with at least one post-baseline MRI. All participants in the study cohort were of European ancestry; 51% were female. The mean age was 70.3 years. 31% had ARIA-E, 19% had ARIA-H microhemorrhage, and 14% had ARIA-H superficial siderosis. We identified one genome-wide significant ( < 5.0 × 10) association at the chromosome 19 locus encompassing . The association with ARIA was stronger in ε4/ε4 homozygotes (OR = 4.28, 4.58, 7.84; < 2.9 × 10 for ARIA-E, ARIA-H microhemorrhage, and ARIA-H superficial siderosis, respectively) than in ε3/ε4 heterozygotes (OR = 1.74, 1.46, 3.14; ≤ 0.03). We found greater odds of radiographically severe ARIA (OR = 7.04-24.64, ≤ 2.72 × 10) than radiographically mild ARIA (OR = 3.19-5.00, ≤ 1.37 × 10) among ε4/ε4 homozygotes. ε4 was also significantly associated with both symptomatic (ε4/ε4 OR = 3.64-9.52; < 0.004) and asymptomatic (ε4/ε4 OR = 4.20-7.94, < 1.7 × 10) cases, although among ARIA cases, did not appear to modulate symptomatic status. No other genome-wide significant associations were found.
We identified a strong, genome-wide significant association between and risk of ARIA. Future, larger studies may be better powered to detect associations beyond These findings indicate that is the strongest genetic risk factor of ARIA incidence, with implications for patient management and risk-benefit treatment decisions.
Both trials (ENGAGE [221AD301]: NCT02477800 and EMERGE [221AD302]: NCT02484547) were registered in June 2015 at clinicaltrials.gov and enrolled patients from August 2015 to July 2018.
在 aducanumab(一种抗淀粉样蛋白单克隆抗体)的 3 期 ENGAGE 和 EMERGE 试验中,最常见的不良事件是淀粉样相关影像异常(ARIA)。先前的 aducanumab 及其他抗淀粉样蛋白治疗试验表明,ε4 携带者状态会增加 ARIA 的风险;然而,尚未评估人类基因组的其余部分是否为 ARIA 的风险因素。因此,我们试图以假设自由的方式确定,在接受 aducanumab 治疗的患者中,除了 以外的遗传变异是否会影响 ARIA 的风险。
我们对 ENGAGE 和 EMERGE 试验中接受 aducanumab 治疗的患者的 ARIA 进行了全基因组关联研究(GWAS)。参与者患有阿尔茨海默病导致的轻度认知障碍或轻度阿尔茨海默病痴呆症,且正电子发射断层扫描(PET)显示淀粉样蛋白阳性。所有参与者均接受定期 MRI 监测以检测和诊断 ARIA。
在意向治疗人群的 3285 名参与者中,本分析纳入了 1691 名接受至少一剂 aducanumab 治疗且至少有一次基线后 MRI 的参与者。研究队列中的所有参与者均为欧洲血统;51%为女性。平均年龄为 70.3 岁。31%有 ARIA-E,19%有 ARIA-H 微出血,14%有 ARIA-H 表浅铁质沉着症。我们在包含 的 19 号染色体位点发现了一个具有全基因组意义的显著关联( < 5.0×10)。在 ε4/ε4 纯合子中,与 ARIA 的关联更强(OR=4.28、4.58、7.84;ARIA-E、ARIA-H 微出血和 ARIA-H 表浅铁质沉着症的 < 2.9×10),而在 ε3/ε4 杂合子中则较弱(OR=1.74、1.46、3.14;ARIA-E、ARIA-H 微出血和 ARIA-H 表浅铁质沉着症的 ≤ 0.03)。我们发现,与影像学轻度 ARIA(OR=3.19-5.00, ≤ 1.37×10)相比,ε4/ε4 纯合子发生影像学严重 ARIA(OR=7.04-24.64, ≤ 2.72×10)的可能性更大。ε4 还与症状性(ε4/ε4 OR=3.64-9.52; < 0.004)和无症状性(ε4/ε4 OR=4.20-7.94, < 1.7×10)病例均显著相关,尽管在 ARIA 病例中, 似乎并未调节症状状态。未发现其他具有全基因组意义的关联。
我们确定了 与 ARIA 风险之间的强烈、具有全基因组意义的关联。未来,更大规模的研究可能更有能力检测到 的关联。这些发现表明, 是 ARIA 发生率最强的遗传风险因素,这对患者管理和风险效益治疗决策具有影响。
两项试验(ENGAGE [221AD301]:NCT02477800 和 EMERGE [221AD302]:NCT02484547)于 2015 年 6 月在 clinicaltrials.gov 上注册,并于 2015 年 8 月至 2018 年 7 月招募患者。